Abnormal Fetal Position and Presentation
Abnormal Fetal Position and Presentation
Fetal position and presentation are both very important when it’s time for labor and delivery. Unborn babies usually spin and flip within their mother’s uterus until a few weeks before delivery. But most babies eventually settle into one position shortly before birth, which is almost always established by the 36th week of pregnancy. Presentation can change or be changed during labor.

Fetal Position vs. Fetal Presentation
People often use the terms “position” and “presentation” interchangeably. While there might be some overlap in meaning, the words refer to two very different things:
- Fetal Position refers to how a baby is lying within its mother’s womb
- Fetal Presentation specifically relates to the part of the baby’s body pointing toward or entering the birth canal at the time of birth
In some cases, ‘position’ becomes ‘presentation.’ For example, a baby that is in a breech position before birth might be a breech presentation at birth. However, babies can move spontaneously into another birth position during labor. Doctors also may attempt to move the baby into a better position before or during labor.

Two Common Fetal Positions
The best position for the unborn child is usually occiput anterior. This medical term means that the baby is head down in its mother’s pelvis facing her spine. Variations of occiput anterior refer to whether the baby is leaning left or right. The baby’s position can affect the best delivery method for mom and infant.

Babies can also be head down but facing the mother’s abdomen. This position is called occiput posterior. With this fetal position, labor is generally longer and more difficult for mother and baby, putting them at risk of labor complications.

Common Fetal Presentations
Doctors (obstetricians and maternal fetal specialists), nurses, midwives, and other obstetrics professionals identify the presentation through ultrasounds and physical examination. Some presentations are dangerous to both the mother and baby. Early diagnosis and intervention are necessary in order to prevent a birth injury, birth trauma, fetal distress and brain damage like hypoxic-ischemic encephalopathy (HIE).
When medical professionals see abnormal fetal presentations, they must take steps to either correct the presentation or closely monitor the baby with follow up ultrasounds and electronic fetal monitoring during labor.

Occiput (head)
The word “occiput” means head. A baby in occiput presentation is emerging head-first. This is usually the best presentation but can be complicated if the head is turned too far to the left or right.
Most complications with occiput presentation occur because the baby is positioned facing outward its mother’s abdomen.
The baby is head-first in two additional presentations: brow and face. However, occiput fetal presentation refers to the top of the baby’s head presenting first.
Brow Presentation
In this type of fetal presentation, the baby’s neck is slightly arched. Doctors, nurses, and midwives will see the baby’s “brow” or forehead instead of the top of the skull.
Sometimes the baby corrects its position before actually presenting. If not, doctors may need to deliver the baby by cesarean section (C-section). The reason for a c-section is because usually the diameter of the head (in the brow presentation) is too wide to fit through the mother’s pelvis. This can cause a prolonged labor, an arrest of labor or birth trauma, all of which can cause a birth injury including hypoxic-ischemic encephalopathy (HIE).
Face Presentation
Sometimes a baby’s neck is so arched that it presents face first. This is not an ideal presentation and can lead to labor complications including prolonged or arrested labor that can cause fetal distress.
Face presentation also puts the baby at higher risk for birth trauma to the face, skull, throat and even spinal cord injury due to the hyperextension.
As with brow presentation, face presentation generally means that the doctor must perform a C-section in order to avoid known birth complications.
After a brow or face presentation birth, the newborn baby might be bruised or swollen. These conditions generally get better within a day or two. In more serious cases, the baby might need neonatal resuscitation or a breathing tube. Doctors delivering a baby in face presentation must be prepared for neonatal resuscitation so that a newborn baby does not suffer from a lack of oxygen (anoxia) shortly after birth.
Breech Presentation
About 3-4% of deliveries are breech presentations, which means the baby’s feet or buttocks enter the birth canal first. Babies that are at breech at 37 weeks of pregnancy will not change on their own from this position. Doctors usually deliver breech babies by C-section because the baby is at risk for:
- Umbilical cord compression, prolapse or nuchal cord (cord around the neck) that can cause a lack of blood or oxygen to the baby
- Spinal cord injuries
- Nerve damage
- Brain damage due to physical birth trauma
- Hypoxic-ischemic injury due to reduced blood and oxygen flow (ischemia or hypoxia) to the infant’s brain
There are several types of breech fetal presentation, including:
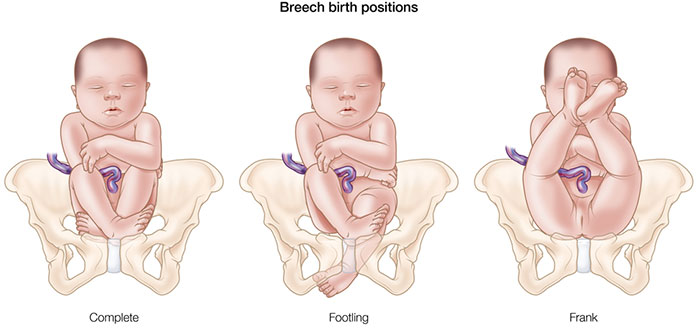
- Complete breech: The baby’s buttocks present downward into the birth canal with hips and knees flexed.
- Frank breech presentation: As with a complete breech, the baby’s buttocks present first. However, the baby’s legs are straight up with their feet near the head.
- Footling breech: One or both of the baby’s feet are being delivered first.
- Transverse lie: Here, the baby is lying sideways in the mother’s uterus. Fetal presentation would be the baby’s shoulder, arm, or hand.
Delivery by Cesarean section is necessary with most breech presentations. Vaginal deliveries are not generally considered safe to attempt due to the high degree of risks and complications due to breech presentation. When a C-section is delayed, the baby can sometimes descend too far into the birth canal and must be delivered vaginally, posing great risk to the mother.
Managing Abnormal Fetal Presentation or Position
Fetal position and presentation are essential pieces of information that doctors, midwives, and nurses must consider. Medical professionals should catch dangerous positions and presentations during prenatal visits using ultrasound or physical examinations. Medical intervention is often needed when position or presentation is not optimal. Failing to diagnose and manage dangerous fetal positions and presentations is medical malpractice.

How doctors handle an abnormal fetal position or presentation depends on several factors:
- Diagnosis – When was the fetal position or presentation noticed?
- Mother’s condition – Does the mother have any medical conditions that make vaginal birth dangerous?
- Baby’s condition – Are there signs of fetal distress?
When doctors diagnose the dangers before labor starts, they may:
- Attempt to move the baby into a more advantageous position. Doctors may perform an external cephalic version, which involves pressing the mother’s abdomen to move the baby into place. There are risks of this maneuver.
- Schedule a C-section when vaginal birth will be dangerous for mother and baby.
- Have the mother deliver in a hospital setting that has the equipment and personnel to handle emergency C-sections and other procedures including neonatal resuscitation.

The situation is even more critical during labor and delivery. Doctors, nurses, and midwives should monitor the mother and baby closely to watch for signs of fetal distress. Careful and thorough physical examinations conducted during labor can identify abnormal presentations that require immediate action.
Complications Due to Fetal Position or Presentation
As with other labor complications, new mothers and their infants can suffer greatly. Their pain and suffering can be more significant when medical providers fail to provide the proper care to them.
After a traumatic birth, women may experience one or more of the following:
- Excessive physical pain as they heal from childbirth
- Longer recovery times
- Post-traumatic stress disorder or
- Post-natal depression

They also may have to accept and deal with birth-related injuries to their babies that could include:
- Excess bruising
- Head and facial molding
- Shoulder dystocia
- Brachial plexus injuries
- Spinal cord injuries
- Hypoxic-ischemic encephalopathy
- Birth Trauma
- Cerebral Palsy
Some injuries like bruising and molding typically resolve without long-term damage to the infant. Babies with nerves, muscles, and spinal cord damage may require physical therapy and surgery before fully recovering.
However, hypoxic-ischemic encephalopathy (HIE) poses a far greater and longer-lasting danger. Hypoxia occurs when oxygen flow is reduced to the unborn baby. Ischemia means that blood flow has been reduced to the baby, which in turn deprives vital organs of the blood and oxygen they desperately need. This can lead to a permanent brain injury including cerebral palsy. If HIE is diagnosed at birth the baby should immediately be evaluated for hypothermia therapy (cooling) to minimize the progression of the brain injury.

Newborns often need neonatal resuscitation and other intense treatments to minimize brain damage. But in many cases, infants have sustained permanent brain damage. HIE is a leading cause of cerebral palsy. Babies may also develop seizure disorders, cognitive and learning disabilities, and developmental delays.
In most cases, medical providers – including obstetricians, family doctors, nurses, and midwives – missed the signs of abnormal fetal position or presentation. Diagnosing and managing the situation is crucial to the mother’s well-being and the baby’s future.
Is Your Child’s Birth Injury the Result of Medical Malpractice?
The parents of children who suffered a birth injury or birth trauma due to fetal position or presentation want answers. They want to know what happened to harm their child. Were there signs of abnormal fetal position or presentation that the doctors and nurses failed to recognize and/or failed to respond to in a timely or correct manner? Did their child suffer permanent brain damage because of medical negligence and malpractice?
Our dedicated birth injury lawyers want to help you find those answers.
We diligently investigate the facts, including a detailed examination of the fetal heart rate monitoring strips and labor and delivery records. If this review shows the medical providers did not diagnose or respond to fetal distress, we hold responsible parties accountable by pursuing medical malpractice claims against them. The compensation our clients receive helps them pay for their child’s current and future medical treatment, assistive technology and equipment, attendant care, and the other expenses associated with caring for a child with brain injuries, seizure disorders, and cerebral palsy.
Sometimes families are afraid to talk to lawyers about their child’s case because they worry there is a fee. There is never a fee unless and until we make money recovery for our clients.

Why Should You Talk with the Knowledgeable Attorneys at Miller Weisbrod?
The only way to find out if you have a birth injury case is to talk to an attorney who understands birth injury.
At Miller Weisbrod Olesky, a team of committed professionals uses our detailed case review process to assess your potential claim. They start by learning more about you and your child. Then we gather medical records to determine what happened before, during, and after your delivery. We call in skilled medical experts who review your records and let us know if they think medical errors could have caused your child’s injuries.
If we feel medical malpractice was present, we meet with you to discuss how you can receive compensation from the medical professionals who made the errors.
At no point in our legal intake process will we ask you to pay anything. The medical review of your case and the consultation are free. We only receive payment when you do.
Contact Miller Weisbrod Olesky
National Birth Injury Law
Our National Birth Injury Attorneys, nurses, and support staff understand that parents of children with birth injuries feel overwhelmed. So, every client has the attention and support of a team of trained, compassionate professionals. But we don’t just offer compassion.
We offer a process to help you discover whether your child’s birth injury, HIE, cerebral palsy or brain injury at birth was caused by medical malpractice.
Call our offices today at (888) 987-0005 for experienced assistance in a free consultation.
Quick Links
Testimonials
- Lyric C. I feel like our voice was heard in a sense of what can possibly go wrong in a delivery and finding us answers. I feel with our settlement, we are now in a comfortable position to provide for our son.
- Lyssa L. They are not just people that say “hey let's get you money and let's go” The law firm was very thorough with us. It was awesome. I don't want to cry, because I think about and it's amazing that they were able to help me and that we were able to help my son and get the story out there.
- Jay C. Throughout the process, one thing was clear to us, the ultimate interest of our child was the utmost concern of Max and his team and as parents navigating a situation like that, that was refreshing to know we had them firmly on our side. I highly recommend them.
Popular Cities
- ★ Dallas Birth Injury
- ★ Houston Birth Injury
- ★ Atlanta Birth Injury
- ★ Chicago Birth Injury
- ★ Philadelphia Birth Injury
Locations
★ Dallas
11551 Forest Central Drive, Ste. 300
Dallas, TX 75243
★ Houston
12929 Gulf Freeway, Ste. 111
Houston, TX 77034