A baby’s heart rate before birth is a critical indicator of their wellbeing. Doctors and other healthcare professionals are held to strict standards when it comes to monitoring fetal heart rate patterns and the decisions they make based off of them.
When fetal heart rate monitoring indicates concerning variability or heart rate decelerations, healthcare providers only have a short window to take action before risking irreparable harm. When an OB-GYN, nurse, midwife, or any other medical professional needlessly delays care during a labor and delivery complication, they may be held liable for committing medical malpractice.
Over the past three decades, the nationally recognized team of birth injury lawyers, registered nurses, and nurse-attorneys at Miller Weisbrod Olesky have established a proven track record of delivering justice for children and families across the United States who have suffered from all types of birth injuries.
We are prepared to meticulously investigate the circumstances of your case, gather crucial medical records, consult with top medical experts, and fight tirelessly to secure the compensation you deserve for your child's birth injury.
We work on a contingency fee basis, meaning you won't pay any legal fees unless we win your case. We only receive payment once you do.
Recent Birth Injury Settlement:
Birth Injury settlement against a hospital in which nurses and physicians failed to properly monitor the mother's blood pressure during delivery causing an HIE event resulting in neonatal seizures and cerebral palsy at birth. Our team of experienced birth injury lawyers recovered $13,750,000 for the family to help with future medical expenses and developmental therapy.
What is Fetal Distress?
Fetal distress (also known as fetal intolerance to labor) is a term that was used for years in the medical field to describe a concerning fetal heart rate. “Concerning” could refer to a fetal heart rate that’s abnormally high, one that’s abnormally low, or a heart rate that is rapidly fluctuating between too high and too low.
Non-reassuring fetal heart rates are fairly common during labor and delivery, estimated to occur between 10% and 25% of pregnancies.
The issue with the term fetal distress is that it’s often imprecise and nonspecific, leaving too much room for interpretation over which heart rate patterns are “distressing” enough to warrant action. This is why, in 1998, the American College of Obstetricians and Gynecologists (ACOG) published a committee opinion piece suggesting for the first time to swap out fetal distress for a more specific term: non-reassuring fetal heart rate status.
Despite being an imperfect term, fetal distress is still the more common and recognizable phrase with the general public to this day for non-reassuring fetal heart rates. We will use the terms interchangeably on this page, but it’s important to note that medical institutions should aim to shy away from diagnosing babies with “fetal distress” because of how broad it can be.
What is a Normal Fetal Heart Rate?
A normal fetal heart rate should rest in between 110 and 160 bpm (beats per minute).
During labor, the baby’s heart rate is carefully tracked using electronic fetal heart rate monitoring equipment. The reading strip comes back in two pieces: the top part of the strip measures the baby’s heart rate, and the bottom part measures the mother’s contractions. Each red line indicates one minute.
A baby’s fetal heart rate can be defined by the following characteristics: the baseline, accelerations, decelerations, and variability.
A baseline fetal heart rate is the baby’s average heart rate over a 10-minute period. This excludes massive jumps or dips in response to contractions. If this baseline is higher than 160 bpm, it is indicative of fetal tachycardia. When the baseline is lower than 110 bpm, it is typically a sign of fetal bradycardia.
An acceleration is a temporary spike in the baby’s heart rate, typically as a response to fetal movement or a contraction. Accelerations are generally considered to be a reassuring sign of the baby’s wellbeing and adequate oxygen supply.
A deceleration is a temporary drop in the baby’s heart rate. Decelerations can either be reassuring or non-reassuring, depending on when and why they occur:
Early decelerations are heart rate dips that line up with the mother’s contractions. This is expected and considered healthy as long as the heart rate jumps back to the baseline afterward.
Late decelerations are heart rate dips that don’t line up with contractions. They occur when the lowest point of the heart rate comes after the peak of the mother’s contraction. This is considered abnormal and can indicate some level of fetal distress.
Variable decelerations are a pattern of heart rate dips that happen suddenly and abruptly. The more frequent variable decelerations are, the more concerning it becomes.
Variability in fetal heart rates refers to the small differences from the baseline rate over several minutes. A baby’s heart rate might accelerate or decelerate but should return to or near its baseline rate. Variability can be classified into several subsections:
Absent variability means there is very little to no change at all in the heart rate. This can be concerning and indicative of oxygen deprivation.
Minimal variability means there are visible fluctuations, but only of 5 bpm or less. Like absent variability, minimal variability can also be concerning and merit further investigation.
Moderate variability means visible fluctuations between 6 and 25 bpm. This is a standard and healthy range of variability and often does not indicate an issue (although other factors may point to one).
Marked variability means there are large fluctuations exceeding 25 bpm. While this isn’t always cause for concern, this variability may indicate an issue when it is prolonged over extended periods.
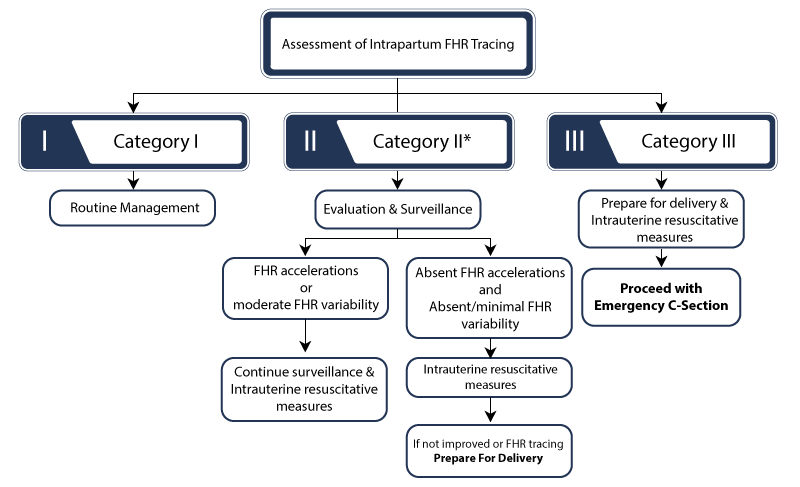
In 2008, a three-tiered classification system was recommended to standardize the management and responses to abnormal and non-reassuring fetal heart rate tracings. Category I heart tracings are considered reassuring, Category III heart rates are considered emergencies, and Category II tracings are usually somewhere in between and require closer evaluation and management.
Fetal heart rates are often dynamic and fluctuating as the baby endures the stress of labor, and they can frequently evolve or shift from category to category over time. A fetal heart rate tracing should be interpreted in the context of the mother’s overall status.
There are instances where fetal heart rates can appear concerning or non-reassuring and the baby ends up being perfectly healthy, but doctors and healthcare providers should always either quickly correct the non-reassuring heart rate tracings or move to delivery in order to protect the child.
However, This complex process must be carefully understood and adhered to so that healthcare providers don’t miss the opportunity to prevent a birth injury or even a wrongful death.
A non-reassuring fetal heart rate status almost always means that the fetus is not receiving adequate oxygenation (the process by which the body’s cells receive oxygen to create energy and survive).
During labor, the mother’s contractions temporarily restrict the flow of oxygenated blood. This process is natural, but a baby can only go so long with diminished oxygenation before they go into birth asphyxia and their heart rate starts to drop.
Two of the most common causes for reduced oxygen are placental complications and umbilical cord problems. The umbilical cord is the baby’s lifeline during pregnancy. Attached to the placenta, the cord is the vessel by which blood, oxygen, and other nutrients travel from the mother to the baby.
When a complication arises to either of these crucial organs, it can compromise the baby’s blood and oxygen supply and put them at risk for hypoxia, asphyxia, and ultimately fetal distress.
Examples of umbilical cord complications include knots, cords wrapping around the baby’s neck, umbilical cord compression, or umbilical cord prolapse (when the cord exits the birth canal before the baby does).
Another common cause of fetal distress is cases of prolonged and arrested labor. Labor is strenuous for not just the mother, but the baby as well. The pressure of contractions on the baby’s head for extended periods can ultimately affect fetal heart rates, especially when coupled with a labor and delivery complication like uterine tachysystole (when contractions occur more frequently than normal).
Certain factors may increase a mother’s chances for having a prolonged or arrested labor. This can include abnormalities in fetal size like macrosomia or cephalopelvic disproportion (when the baby’s head is too large to fit through the mother’s birth canal). The baby may also be in an abnormal fetal position that makes progressing through the birth canal more difficult or even impossible, such as breech position or shoulder position.
Another common cause for prolonged labor is when the mother starts out with having weak contractions (known as hypotonic labor). When this happens, medical providers will typically try to induce labor using medications like Pitocin and Cytotec.
These medications can successfully induce labor contractions when used correctly, but sometimes an overdosage can have the opposite effect and induce contractions that are too frequent and too forceful. This is known as uterine hyperstimulation, and the overly forceful contractions can prolong labor even further and put an unsafe amount of pressure on the baby.
The baby’s heart rate will in turn respond by rapidly decelerating when the contractions cut off oxygen flow to unsafe levels for too long.
Which Risk Factors Increase the Threat of Fetal Distress?
Certain maternal conditions and pregnancy complications can increase the chances of fetal distress. Examples of this include:
Gestational Diabetes: Having maternal diabetes during pregnancy increases the chances of fetal size abnormalities like macrosomia or cephalopelvic disproportion, which will make labor more strenuous and possibly dangerous for fetal heart rates.
Preeclampsia: The abnormally high blood pressure that comes with preeclampsia has the potential to impair placental function and cause disruptions in oxygenated blood flow to the baby’s heart and brain, increasing the risk of fetal distress.
Maternal Infections: When left untreated or insufficiently treated, maternal infections like group B strep or chorioamnionitis have the potential to transfer to the baby in utero. At that point, it becomes a neonatal infection and can cause multiple complications for the baby, including inflammation, an increased fetal heart rate (tachycardia), and prolonged decelerations.
Post Term Pregnancy: A pregnancy that goes past the anticipated due date can put the mother at risk for placental insufficiency.
The placenta is a temporary organ meant to be expelled after the baby is fully developed, and it commonly begins to weaken and deteriorate after the mother’s due date passes.
This can be troubling when the baby still has not delivered yet, because they are then losing their source of oxygen and nutrients while still in the womb, which can negatively impact fetal heart rates.
The signs of fetal distress can occur even before labor and delivery has started. For example, if the mother notices a lack of fetal movement during pregnancy, it can sometimes indicate that something isn’t right. The mother may also notice bleeding during the later stages of her pregnancy, which can sometimes be a sign of a complication like a placental abruption or uterine rupture.
Another common sign of an issue during pregnancy is if the mother notices her stomach isn’t growing enough. This can be a sign of intrauterine growth restriction (IUGR) and indicate that there may be a issue with the placenta or umbilical cord that’s preventing growth and thus affecting the baby’s heart rates.
On the actual heart rate strips themselves, signs of fetal distress can include:
Lack of variability: A healthy baby has moderate variability of their heart rate, varying from 6 to 25 beats per minute. If the fetal heart monitor strips show a lack of variability, then this is a sign of fetal distress. These conditions are known as minimal or absent variability. Loss of variability, especially in the presence of other periodic patterns during labor, is the most sensitive indicator of metabolic acidemia resulting from fetal distress.
The fetal heart rate is too slow: A decreased fetal heart rate can indicate fetal acidosis and other conditions that lead to a non-reassuring fetal status.
Late or prolonged decelerations: Alarming patterns of variable decelerations and late decelerations of the baby’s heart rate can appear during labor. Late decelerations are indicators of fetal distress because the baby is not recovering from the temporary blockage of oxygen during a contraction.
Fetal bradycardia or tachycardia: When the baby’s baseline heart rate falls outside of the 110 to 160 bpm threshold, it can be a sign of some external factor causing distress.
OB-GYNs, nurses, and all other medical professionals involved in the mother’s delivery must closely monitor her contraction patterns and the baby’s fetal heart rate response as it can evolve by the minute and leave very little time for critical intervention.
What Injuries Can Arise from Fetal Distress?
A baby with a non-reassuring fetal heart rate status is grounds for emergency medical intervention. The potential injuries and birth complications stemming from fetal distress are severe, ranging from permanent brain injuries to death. Some of the most serious potential injuries include:
Non-reassuring fetal heart rates typically indicate oxygen deprivation. When the baby’s source of oxygen is completely cut off, it is known as birth asphyxia. All organ systems in the body are interconnected; when birth asphyxia deprives the brain of oxygen, it can cause damage to other vital organs as well.
For the heart, asphyxia can cause lower blood pressure and even be a precursor for cardiac arrest. The lungs will also suffer from lower oxygen levels, leading to breathing difficulties at birth like respiratory distress syndrome (RDS).
Birth asphyxia can also make it more difficult for the liver to produce proteins that assist with blood clotting, which can lead to bleeding and other difficulties with the blood system like anemia and low platelet counts.
If a child is at risk for serious birth injuries like HIE, the fetal heart rate monitoring strips will likely reflect this risk with either rapid decelerations, marked variability, absent variability, or other patterns recognized as abnormal and non-reassuring.
Cerebral palsy is a complex movement disorder made up of multiple physical conditions that affect a child’s motor function, posture, and physical and cognitive development. It is not diagnosed at birth, but normally within the early childhood years.
In extreme cases, non-reassuring fetal heart rates can lead to fetal demise (also known as a stillbirth). If the child is born breathing, then passes away shortly after due to breathing problems like respiratory distress syndrome, then it is classified as infant death.
In most instances of fetal distress, the baby’s death can be prevented if a normal heart rate patterns are detected quick enough and action is taken immediately.
How to Treat Fetal Distress?
Once monitoring and tests indicate the possibility of fetal distress (either a Category II or Category III tracing), medical professionals must act quickly. Failing to do so can cause permanent damage to the baby’s brain, heart, and other organs.
Some treatments for oxygen deprivation include:
Intrauterine resuscitation
Providing additional fluids to the mother
Providing supplemental oxygen to the mother
Moving the mother into a more favorable position for delivery
Amnioinfusion to increase amniotic fluid in the event of oligohydramnios
Fetal heart rates can be unpredictable at times; there are cases where abnormal patterns end up not resulting in any physical harm to the baby upon birth.
Because of this unpredictability, there is no definitive method known to prevent non-reassuring fetal heart rates. The next best possible course of action is to identify when a pregnancy is high risk and to keep a note of potential risk factors and complications that will increase the child’s chances of experiencing fetal distress.
This begins with proper prenatal testing and using the following methods to examine heart rates and other important fetal characteristics throughout the course of the mother’s pregnancy:
Healthcare providers should use all the knowledge and tools at their disposal to prevent and treat complications that may affect fetal heart rates during pregnancy and during labor.
Is Your Child’s Birth Injury the Result of Medical Malpractice?
It is the duty of healthcare professionals to accurately assess the mother’s risk during pregnancy and delivery and take the proper action to mitigate that risk. Sometimes, however, they miss critical signs of issues or fail to act in a timely manner to treat fetal distress. Examples of medical negligence relating to abnormal fetal heart rates include:
Prescribing too high of a dosage of labor-inducing medications resulting in uterine hyperstimulation. This also includes not lowering the dosage after problems are identified.
It’s important to note that it requires a detailed review of the specific facts of the mother’s pregnancy and delivery before making a definitive judgement as to whether medical malpractice played a factor in their child’s birth injuries.
Was My Child’s Birth Injury Preventable?
Birth injuries caused by fetal distress are often life changing. The parents of injured children might seek compensation from negligent healthcare providers. The money they receive cannot take away the birth injury, but it can provide the financial means needed for medication, surgery, therapy, assistive devices, and caregivers.
A baby’s birth injury after undergoing fetal distress isn’t always preventable, but every second counts when it comes to treatment. Medical negligence, such as failing to properly read and monitor fetal heart rate monitoring strips or needlessly delaying an emergency C-section delivery, can increase the odds the baby sustaining an irreversible birth injury.
Parents whose children suffer from the long term effects of fetal distress injuries like hypoxic-ischemic encephalopathy and cerebral palsy deserve to know whether it could have been prevented. Our dedicated birth injury lawyers want to help you find those answers and obtain the funds necessary to improve your child’s quality of life.
If your child has been diagnosed with an injury that traces back to oxygen deprivation at birth, and you believe that it was caused in part by medical errors, our firm will thoroughly investigate the facts and hold the responsible medical providers accountable by pursuing medical malpractice claims against them.
Sometimes families are hesitant to reach out to a birth injury malpractice attorney or law firm. They may feel overwhelmed by their circumstances or are worried that a law firm will not be able to help them.
But the only way to find out if you have a case is to talk to an attorney who understands how birth injuries can lead to developmental delays and other complications that require long-lasting medical support and treatment.
What is the Statute of Limitations in a Birth Injury Case?
A statute of limitations (SOL) is a law that sets a time limit on how long an injured person has to file a lawsuit after an accident. It is essential to understand that statutes of limitations vary based on the type of case and the state where it is filed. For instance, the deadline for birth injury claims is typically different from other claims, such as injury to personal property, fraud, contract disputes, and collection of debts.
Generally, the clock starts ticking on the date the injury occurred. However, there are exceptions to this rule, and in some cases, the statute of limitations starts when a person discovers or reasonably should have discovered an injury. When dealing with government agencies, SOLs can become even more complex.
For example, if the party that injured you was:
A federal employee
Employed by a military hospital, Veterans Administration facility, or a federally funded medical entity
You may need to file a birth injury claim under the Federal Tort Claims Act (FTCA). In FTCA cases, claimants must go through certain administrative procedures before filing a lawsuit. In some states, if the negligent party was a local or state government hospital or the doctors and medical providers are employees of a governmental entity, the time period in which you must give "notice" may be shorter.
If your case is filed outside of the statute of limitations, it will typically be dismissed, and you will not be eligible to recover compensation for your injuries. Determining when a statute of limitations begins on your case can be tricky. If you're considering pursuing compensation for a birth injury, contacting an attorney as soon as possible is in your best interest.
How The Birth Injury Attorneys at Miller Weisbrod Olesky Can Help
It takes a detailed expert review of the facts and circumstances of your pregnancy and your child's birth before determining whether their birth injury came as the result of mismanaged fetal distress.
At Miller Weisbrod Olesky, a team of committed attorneys, nurses and paraprofessionals uses our detailed medical negligence case review process to assess your potential medical malpractice case. We start by learning more about you and your child and the status of meeting/missing developmental milestones.
Then we gather medical records to determine what happened before, during, and after your delivery. We call in skilled medical experts who review your records and let us know if they think medical errors could have caused your child's injuries.
If we feel medical negligence caused or contributed to your baby’s fetal distress and resulting birth injury, we meet with you to discuss how you can receive compensation from the medical professionals who made the errors.
At no point in our legal intake process will we ask you to pay anything. The medical review of your case and the consultation are free. We only receive payment when you do. The sooner you reach out to us, the sooner we can begin investigating your case and gathering the evidence needed to support your claim.
We work on a contingency fee basis, meaning you won't pay any legal fees unless we win your case. Contact us today to schedule your free legal consultation by calling our toll-free line at (888) 987-0005 or by filling out our online request form.
Contact Miller Weisbrod Olesky
National Birth Injury Law
Our National Birth Injury Attorneys, nurses, and support staff understand that parents of children with birth injuries feel overwhelmed. So, every client has the attention and support of a team of trained, compassionate professionals. But we don’t just offer compassion.
Lyric C. I feel like our voice was heard in a sense of what can possibly go wrong in a delivery and finding us answers. I feel with our settlement, we are now in a comfortable position to provide for our son.
Lyssa L. They are not just people that say “hey let's get you money and let's go” The law firm was very thorough with us. It was awesome. I don't want to cry, because I think about and it's amazing that they were able to help me and that we were able to help my son and get the story out there.
Jay C. Throughout the process, one thing was clear to us, the ultimate interest of our child was the utmost concern of Max and his team and as parents navigating a situation like that, that was refreshing to know we had them firmly on our side. I highly recommend them.