Delayed C-Section Errors
Cesarean Section Deliveries & Birth Injuries

Most babies enter this world through a vaginal birth. This means they exit their mother’s womb via the cervical opening and push out headfirst through her birth canal.
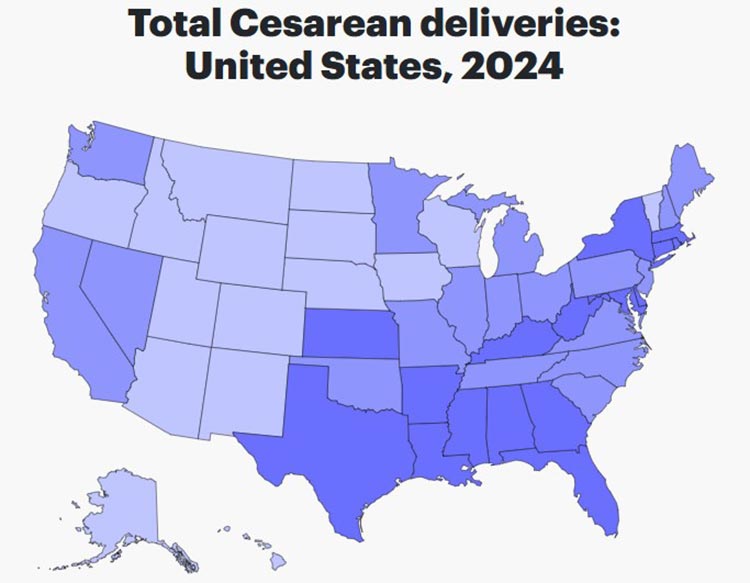
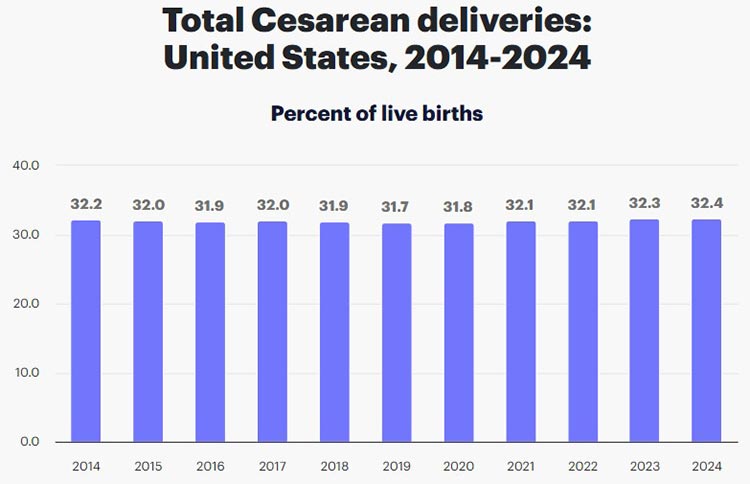
Since the beginning of humanity, people have regarded this as the “natural” way of giving birth. But in recent years, C-section deliveries have emerged as an increasingly common delivery method. In fact, doctors delivered just under a third of all babies in the U.S. by C-section in 2024.
C-section procedures offer a safer delivery method for expecting mothers with high-risk pregnancies. They can also be a lifesaving backup plan if emergency labor and delivery complications threaten the mother’s or baby’s lives.
C-section deliveries carry higher risks than a typical vaginal birth. It is critical that doctors, nurses, and other delivery room professionals act with extreme caution in a timely manner. Needlessly delaying the procedure can prolong an unborn baby’s oxygen deprivation and open the door for irreversible brain injuries.
Delayed C-sections are a significant cause of hypoxic ischemic encephalopathy (HIE), the most common type of brain damage at birth. HIE injuries at birth can cause a wide variety of developmental delays and movement disorders like cerebral palsy. When a child sustains these injuries because doctors waited too long to perform a C-section, it qualifies as medical malpractice.
Birth Injury Malpractice Attorneys
Medical errors can set the tone for the rest of a baby’s life when they cause permanent, irreversible birth injuries. Even seemingly small mistakes like delaying an emergency C-section can have life-altering consequences. Our national c-section birth injury attorneys help these children seek justice by pursuing medical malpractice claims against the responsible parties.
Free Legal Consultation
Birth Injury Malpractice Lawyers
(888) 987-0005Our Birth Injury Malpractice Lawyers are available to meet you in your home or the hospital, nationwide.
We are available today to assess the strength of your claim and whether your family is eligible to recover financial damages. We can answer complex legal and medical questions during our free consultation and intake process.
If you decide to hire us, we will provide you with not just an attorney but an entire medical team. Unlike other firms, we have a vast network of medical experts, in-house nursing staff, and nurse-attorneys assigned to every case.
Our firm understands that your child’s needs cannot simply go on hold while your case is ongoing. This is why we offer financial help and medical assistance immediately, not just after we win.
As your attorneys deal with the litigation process, your medical team will ensure your child receives the care they need. This includes assistance with obtaining medical records, scheduling doctors’ appointments, providing transportation, and any other problems that may arise.
We offer these services on a contingency fee basis. This means that you do not pay a single penny out of pocket until after we win your case. When we win, we will only charge a pre-agreed percentage in fees from your settlement or jury award.
Our c-section birth injury team has recovered hundreds of millions in compensation for our clients. Our track record of birth injury results speaks for itself.

Recent C-Section Case
After a mother suffered a uterine rupture during delivery, doctors failed to perform a timely C-section. This led to the infant suffering from permanent brain damage at birth. Our team of top rated birth injury lawyers recovered $3,000,000 to help with future medical expenses and therapies.
What is a C-Section?
A Cesarean section (C-section) delivery is a medical procedure where doctors manually deliver the baby from the mother’s uterus. They make a small incision into her lower abdomen and uterus and then reach in to remove the child.

A mother may schedule her C-section in advance when she has known pregnancy complications that will make vaginal birth unsafe. Other times, it becomes necessary to perform an emergency C-section during delivery when unforeseen complications arise.
How Common Are C-Sections?
In 2024, around 32.4% of live births in the United States were C-sections. This figure has remained relatively steady over the last decade, according to maternal healthcare research group March of Dimes.
When Are C-sections Necessary?
C-sections become medically necessary when complications block vaginal birth from being safe to attempt. Sometimes a mother knows about these complications in advance, and other times they appear unexpectedly during labor.
Reasons for a Planned C-Section

A mother may plan her C-section in advance when medical providers make any of the following discoveries during prenatal testing:
- The baby is in an abnormal fetal position like breech or shoulder position
- The mother has placenta previa (when her placenta covers the top of the cervical opening)
- The mother is carrying twins or multiple babies
- The baby is larger than 4000 grams and may not fit through the birth canal (fetal macrosomia)
- The baby’s head is too large to fit through the mother’s pelvis (cephalopelvic disproportion)
- The mother has concerning pregnancy complications like preeclampsia or HELLP syndrome
- The mother has infections affecting her urinary tract (genital herpes, E. Coli, etc.)
- The mother has had multiple C-sections in the past
- The mother has had previous uterine procedures that increase her risk of a uterine rupture
Reasons for an Emergency C-Section

Some mothers do not have the luxury of a planned C-section. Instead, complications during labor and delivery drive the need to deliver via C-section. Medical professionals in the delivery room should waste zero time preparing for a C-section when the following emergencies occur:
- The mother’s labor becomes prolonged or arrested (12-14 hours without progression)
- The baby experiences umbilical cord problems like cord compression or prolapse
- The baby shows signs of serious fetal distress like late decelerations or fetal bradycardia
- The mother’s placenta prematurely detaches from the uterine lining (placental abruption)
- The mother’s uterus ruptures during delivery
How Long Does a C-Section Take?
A standard C-section delivery takes around 30-60 minutes to complete, with emergency procedures being even faster. Doctors and delivery nurses should deliver the baby within the first 10 to 15 minutes or less of the procedure.
Here’s what the entire process should look like, from beginning to end:
Step 1: Preparation
If the mother has a planned C-section, her healthcare providers will outline the procedure details ahead of time. She will usually need to sign a consent form acknowledging the potential risks.
IMPORTANT NOTE
You may still have a viable birth injury medical malpractice claim even if you signed a C-section consent form. Acknowledging the associated risks of the procedure does not excuse negligent mistakes that directly harm you or your baby.
Before the operation, medical professionals will lay the mother down and make sure she’s comfortable. They will insert a catheter to keep her bladder empty, and they may provide supplemental oxygen through a mask. This is to maintain steady oxygen flow to the baby.
An anesthesiologist will insert an IV to administer regional anesthesia, usually in the form of an epidural. This will keep the mother awake but numb all of her pain in the area before the procedure.

Medical providers sometimes use general anesthesia in emergency C-sections. This allows them to begin surgery faster, but it means the mother will be unconscious for the baby’s birth.
As the mother receives anesthesia, healthcare providers must carefully monitor her vital signs like heart rate and blood pressure. They must also keep a close eye on the baby’s fetal heart rates for indicators of fetal distress.
Step 2: Delivery
After covering the mother’s body with a sterile drape, medical professionals will prep her abdomen for incision. They will disinfect the area with antiseptic and shave any surrounding body hair.
Then, the surgeon takes over and makes a 3-to-4-inch incision into the mother’s abdomen.
Different Types of C-Section Incisions
There are three general types of C-section incision:
- Low transverse: The incision runs horizontally across the mother’s lower abdomen.
- Low vertical: This incision goes from near the center of the mother’s lower abdomen toward the belly button.
- Classical: The classical incision runs across the middle of the mother’s abdomen.

The surgeon then cuts into the mother’s uterus. They will suction out amniotic fluid and gently pull the baby out through the incision site.

Immediately upon delivery, medical providers will suction the baby’s airway to remove any remaining amniotic fluid. In a vaginal birth, babies naturally expel this fluid as the mother’s contractions push them through the birth canal. This is why babies born by C-section often need extra suctioning.
Other times a baby must receive suctioning because they have inhaled meconium (the first stool). Failure to suction a baby when meconium is present at birth can result in meconium aspiration syndrome (MAS) and asphyxia.
Step 3: Aftercare
After delivery, the surgeon will need to remove the mother’s placenta from her uterus. They will clean the area and soak up any excess blood loss before stitching up the incisions.
Doctors will use dissolvable stitches for her uterus and abdominal muscles, and they typically close the outer skin with staples. These staples will stay in for around a week post-surgery before a healthcare provider manually removes them.
Most mothers will spend 2 to 3 days in the hospital recovering from the C-section. It can take up to several weeks for abdominal pain and soreness to subside.
Medical professionals must pay careful attention to the mother’s needs after her C-section. It is their job to keep her as comfortable as possible and best prepare her for recovery. They must stay alert for common risks such as infections or blood clots following the procedure.
How Can Delayed C-Sections Cause Brain Damage?

One of the main reasons for emergency C-sections is because the baby is not responding well to labor.
Uterine contractions naturally squeeze against the baby and the placenta during labor, which constricts oxygenated blood flow. Babies can withstand a certain degree of diminished oxygenation, but abnormally strong contractions or prolonged labor can quickly turn deadly.
The baby’s brain cells start to die off when they do not have enough oxygenated blood to produce energy. This rapid cell death causes inflammation in the brain tissue, leading to permanent brain injuries like hypoxic ischemic encephalopathy (HIE). HIE injuries are the leading cause of cerebral palsy, a group of neurological disorders affecting a child’s muscle movement.
Once a baby develops brain injuries like HIE, it becomes impossible to “undo” them. These birth injuries will dramatically alter a child’s life trajectory, and they can stem from avoidable delays in emergency care.
Possible reasons why healthcare providers may delay emergency C-sections include:
- They do not have the necessary resources to perform a C-section
- There is miscommunication between medical personnel over the need for a C-section
- They are mistakenly encouraging the mother to continue attempting vaginal birth
- They are not properly monitoring the baby’s fetal status
How Long Should Doctors Take to Decide?
The American College of Obstetricians and Gynecologists once recommended that emergency C-sections start within 30 minutes after deciding to operate. But in recent years, ACOG has withdrawn the “30-minute rule” recommendation after finding minimal evidence to support its effectiveness. In reality, a baby with severe hypoxia showing Category III heart rate tracings needs intervention within closer to 15 minutes.
Preventing Brain Injuries with Fetal Heart Rate Monitoring
Doctors and nurses can avoid these tragic outcomes by responding as quickly as possible to non-reassuring fetal heart rates.
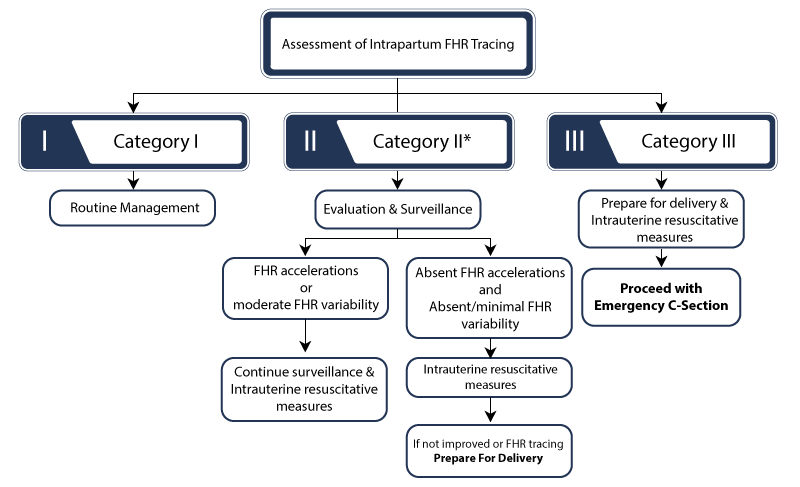
A trained medical professional will be able to categorize fetal heart rate patterns based on several factors. These can include the heart rate’s baseline, variability, and the timing between accelerations and decelerations.
Failing to recognize the signs of a Category II or Category III fetal heart rate can lead to delayed responses. In some cases, it can delay an emergency C-section procedure after the damage has already set in to the brain.
What Are Other C-Section Errors?

While delaying the procedure is the most common error, medical professionals can additionally make other mistakes when performing a C-section. These mistakes can include:
- Anesthesia Errors: Anesthesiologists may administer the incorrect dosage to the mother before the procedure. This can cause breathing issues, maternal brain damage, or sudden drops in blood pressure. Anesthesia errors are a significant risk factor for maternal mortality.
- Surgical Errors: Surgeons can make errors when cutting into the mother’s abdomen or uterus. Cutting too deep into the uterus can injure the baby, and improper cuts can injure nearby maternal organs. Improper use of the scalpel can cause severe bleeding and increase the mother’s risk for a postpartum hemorrhage.
- Post-Op Errors: Improperly stitching up the mother’s wound can increase her risk for future uterine ruptures. Messy incisions without proper cleaning afterward can also increase the likelihood of developing a maternal infection.
Medical professionals can also make errors when removing the baby, especially when using delivery tools like forceps and vacuum extractors. When obstetricians and delivery nurses use excessive force during the C-section, babies can suffer the following injuries:
- collar bone fractures
- brachial plexus injuries
- skin lacerations
- skull fractures
- facial nerve palsy
- cephalohematoma or bruising to the baby’s head
Frequently Asked Questions About C-Sections
Most new mothers experience bleeding for around 3 to 6 weeks after their C-section procedure. While each person is different, this timeline is similar for all mothers regardless of their delivery method.
This is because the postpartum bleeding isn’t actually blood, but rather a light-reddish vaginal discharge called lochia. Lochia is a mixture of blood, mucus, and uterine tissue that results naturally from the uterus shedding its internal lining.
The first stage of lochia after birth will appear darker in color and may contain small blood clots. Some women have compared the first week postpartum to a heavy period cycle. During the second and third stages, bleeding will become thinner and lighter in color before ceasing.
At the incision site on her abdomen, the mother may experience slight bleeding within the first 24 hours. She is usually still recovering in the hospital during this time. Any abdominal bleeding after that is abnormal and warrants further inspection from a medical professional.
The mother should contact her healthcare provider if her vaginal bleeding continues past 10 weeks.
Yes, many women often choose to have a C-section (known as an elective Cesarean procedure).
Planned C-sections are routine in high-risk pregnancies where the mother knows beforehand that vaginal birth will be unsafe. Common pregnancy complications that call for planned delivery include macrosomia, placenta previa, or abnormal fetal positioning.
But an expecting mother can choose to have a C-section even when it isn’t medically necessary. She may make the decision with her healthcare team for convenience, comfort, or other reasons she feels is important.
If the mother decides she wants an elective C-section, her doctors are responsible for informing her of the risks. While C-sections are generally safe, they come with longer recovery times and can be harder on the mother’s body overall.
Yes, C-section procedures are generally safe. In some situations, they are even safer than vaginal birth would be.
C-sections admittedly come with real risks for postpartum complications, such as hemorrhaging, infection, and blood clots. These risks (alongside longer recovery times) are why most doctors recommend vaginal birth in a pregnancy without complications.
However, with proper guidance and management from her healthcare provider, the mother can fully recover without any issues.
Excess swelling after a C-section (normally the result of higher fluid retention and blood volume) will naturally ease over time. Swelling is more common in the lower body, including the abdominal area, legs, ankles, and feet.
Most mothers will notice a decrease in swelling within the first 2 weeks postpartum. However, some will experience longer periods with excess water weight, usually upwards of several months. To reduce excess swelling, many healthcare professionals recommend elevating the legs, wearing compression socks, and staying properly hydrated.
It’s important to note that pregnancy can cause multiple bodily changes that last long after giving birth. Changes in weight or appearance that a mother attributes to swelling may actually be structural alterations from the birthing process.
When the mother has a planned C-section, she has the advantage of preparing beforehand for maximum comfort.
The mother should prepare to stay in the hospital post-op for at least 1 to 2 days. She can prepare by packing an overnight bag with clothing, snacks, and things to keep her comfortable during her stay.
Doctors will advise the mother to avoid solid foods in the 6-8 hours leading up to the procedure. They will also ask her to refrain from shaving or applying any hair products, lotions, perfumes, or deodorant.
Before the procedure begins, medical professionals will do prep of their own. They will insert a catheter and an IV to administer regional anesthesia. They will make any other necessary preparations to get the mother’s body ready for the C-section.
Medical professionals failing to adequately prepare for the C-section can qualify as medical malpractice when it causes preventable injuries.
C-section recovery takes longer than vaginal birth and will look slightly different for everyone. Most mothers can expect to return to their daily routine after 6 to 8 weeks. Expecting mothers who are still struggling to restore full functioning after three months should consult with a doctor.
However, it’s important to keep in mind that all pregnancies can cause permanent bodily changes in appearance. A mother returning to her pre-pregnancy weight is not always a realistic part of every recovery journey.
Your doctor will assess your recovery during routine scheduled check-ups in the months after giving birth. Anyone concerned with their recovery following a C-section delivery should reach out to their primary care provider.
New mothers who are recovering from a C-section should avoid the following activities for at least several weeks:
- Driving
- Lifting objects heavier than the weight of her baby
- Rigorous exercise, especially core/abdominal work (low-intensity activities like walking are fine)
- Climbing stairs
- Sitting in baths, hot tubs, or swimming
A mother’s primary care provider may make additional recommendations, such as avoiding high processed foods or using certain cleaners.
While there is no set limit on the number of C-sections someone can have, each subsequent procedure comes with risks.
One concern is that the mother’s placenta will embed into the uterine scar, a placental complication called placenta accreta. This complication can increase a mother’s risk for postpartum hemorrhage.
However, mothers who have had a previous C-section may actually have more risk attempting vaginal birth afterward. A vaginal birth after C-section (VBAC) can increase the mother’s risk for uterine ruptures and birth complications for the baby.
Any mother who has previously delivered via C-section must consult with her doctor closely when deciding on future delivery methods.
Did a Delayed C-Section Cause My Child’s Brain Injury?

C-sections are lifesaving procedures made possible by modern advancements in maternal healthcare. But the timing of the procedure can mean the difference between life and death for the mother and her baby.
Birth complications are more common after a C-section than with vaginal birth. Negligent healthcare providers may attempt to brush off your child’s injuries as an unavoidable consequence of this risky procedure. But our dedicated c-section related birth injury lawyers will get to the root cause of your child’s injuries.
If a family believes medical negligence worsened their child’s brain damage at birth, legal support may be an option. A specialized birth injury attorney can review the medical records and circumstances to assess whether a claim exists.
We will carefully review what happened minute-by-minute in the delivery room during your labor. We will review fetal heart rate strips and any labor and delivery complications you experienced. If we discover that doctors needlessly delayed an emergency C-section, we will hold them accountable by pursuing birth injury medical malpractice claim.
What Is the Statute of Limitations in a Birth Injury Case?
A statute of limitations (SOL) is a law that sets a time limit on how long an injured person has to file a lawsuit after an accident.
It is essential to understand that statutes of limitations vary based on the case and the state where you file. For instance, the deadline for birth injury claims is typically different from other claims, such as injury to private property.
Generally, the clock starts ticking on the date the injury occurred. However, there are exceptions to this rule. In some cases, the statute of limitations starts when a person discovers or reasonably should have discovered an injury. When dealing with government agencies, SOLs can become even more complex.
For example, if the party that injured you was:
- A federal employee
- Employed by a military hospital, Veterans Administration facility, or a federally funded medical entity
You may need to file a birth injury claim under the Federal Tort Claims Act (FTCA). In FTCA cases, claimants must go through certain administrative procedures before filing a lawsuit. In some states, you may have less time to give notice if:
- The negligent party was a local or state government hospital
- The doctors and medical providers are employees of a governmental entity
If you file your case outside of the statute of limitations, the court will typically dismiss it. This means you will not be eligible to recover compensation for you or your child’s injuries.
Determining when a statute of limitations begins on your case can be tricky. Our national birth injury lawyers can help inform you of all the important filing cutoff dates in your state. We will help your family seek justice and compensation for preventable injuries to you or your baby.
How Can Our Birth Injury Attorneys Help?

The only way to find out if you have a birth injury case is to talk to an attorney who understands how they happen. The compensation our clients receive helps them pay for their child’s current and future medical treatment. This can include:
- Assistive technology and equipment
- Physical therapy, occupational therapy, and/or speech therapy
- Medication prescriptions
- In-home caregivers
- Other expenses associated with caring for a child with brain injuries, seizure disorders, and cerebral palsy
Our Process
Our team of committed birth injury experts uses our detailed case review process to assess your potential claim. We start by learning more about you and your child. We will gather medical records to determine what happened before, during, and after your delivery. We call in skilled medical experts who review your records and let us know if they think medical errors could have caused your child’s injuries.
We will work to hold responsible parties accountable in a C-section negligence lawsuit case by pursuing birth injury malpractice claims against them.
At no point in our legal intake process will we ask you to pay anything. The medical review of your case and the consultation are free. We only receive payment once you do. The sooner you reach out, the sooner we can investigate your case and gather evidence to support your claim.
Contact us today to schedule your free legal consultation by calling our toll-free line at (888) 987-0005. You can also reach us by filling out our online request form.
National Birth Injury Law
Our National Birth Injury Attorneys, nurses, and support staff understand that parents of children with birth injuries feel overwhelmed. So, every client has the attention and support of a team of trained, compassionate professionals. But we don’t just offer compassion.
We offer a process to help you discover whether your child’s birth injury, HIE, cerebral palsy or brain injury at birth was caused by medical malpractice.
Call our offices today at (888) 987-0005 for experienced assistance in a free consultation.
Quick Links
Testimonials
- Lyric C. I feel like our voice was heard in a sense of what can possibly go wrong in a delivery and finding us answers. I feel with our settlement, we are now in a comfortable position to provide for our son.
- Lyssa L. They are not just people that say “hey let's get you money and let's go” The law firm was very thorough with us. It was awesome. I don't want to cry, because I think about and it's amazing that they were able to help me and that we were able to help my son and get the story out there.
- Jay C. Throughout the process, one thing was clear to us, the ultimate interest of our child was the utmost concern of Max and his team and as parents navigating a situation like that, that was refreshing to know we had them firmly on our side. I highly recommend them.
Popular Cities
- ★ Dallas Birth Injury
- ★ Houston Birth Injury
- ★ Atlanta Birth Injury
- ★ Chicago Birth Injury
- ★ Philadelphia Birth Injury
Locations
★ Dallas
11551 Forest Central Drive, Ste. 300
Dallas, TX 75243
★ Houston
12929 Gulf Freeway, Ste. 111
Houston, TX 77034