Pregnancy is a time of excitement, but the birthing process is a sensitive period, and the slightest complication can turn a moment of joy into one of fear and uncertainty. Although a small amount of maternal bleeding at some point during pregnancy and delivery is common, especially in the first trimester, it can also be a sign of a more serious issue. A light amount of vaginal bleeding early in a woman's pregnancy is normal and often not a cause for concern. In fact, many women who experience spotting or bleeding during this time go on to have normal pregnancies and deliver healthy babies.
Bleeding later in pregnancy or heavier bleeding that requires a sanitary pad isn't normal and may indicate a potential complication. If you are bleeding at any stage in your pregnancy, you should call your doctor or midwife. They can help you determine why you are bleeding and offer guidance and support. When physicians and other healthcare providers fail to promptly recognize and address maternal bleeding, it can lead to severe complications such as placental abruption, placenta previa, preterm birth, and uterine rupture.
In such cases, contacting an experienced medical malpractice attorney who can provide you answers as to whether you have a viable claim and help you seek compensation for any injury-related damages can make all the difference for your child and family.
At Miller Weisbrod Olesky, our knowledgeable and compassionate birth injury lawyers understand the emotional and financial burden that can arise when maternal bleeding is not properly treated. With the help of our in-house team of registered nurses and nurse-attorneys, we will thoroughly investigate the circumstances surrounding your pregnancy and delivery, gather supporting evidence, and consult with medical experts to build a strong case on your behalf.
What is Maternal Bleeding During Pregnancy?
The cervix may bleed more easily during pregnancy because blood vessels are developing in this area. Bleeding or spotting is especially common in the first three months (first trimester) and occurs in 15 to 25 in 100 pregnancies. Although bleeding in pregnancy doesn't always mean there is a problem, becoming familiar with the cause of bleeding can provide peace of mind and enable an expectant mother to make informed decisions like contacting her medical provider.
Spotting vs. Bleeding During Pregnancy
Spotting (light bleeding) during pregnancy happens when a woman has a few drops of blood on her underwear. If a woman puts on a panty liner, the blood should not soak through it and will usually go away on its own. Bleeding occurs when the flow of blood is heavy enough that a woman may need a pad to keep it from ruining her underwear.
Depending on when the bleeding occurs, spotting or bleeding during pregnancy can be caused by many factors. It is common for light bleeding or spotting to occur 10 to 14 days after conception. This spotting often happens when the fertilized egg (embryo) implants in the lining of the uterus (endometrium). There are several other causes of maternal bleeding during pregnancy and delivery, which is why it is essential for pregnant women to consult with their healthcare provider if they experience any bleeding or spotting. A medical professional can conduct a thorough investigation, determine the underlying cause, and provide appropriate treatment.
Causes of Bleeding During Maternity
Bleeding during pregnancy can be a cause of concern for expectant mothers. In some cases, maternal bleeding during pregnancy can be a symptom of complications such as an ectopic pregnancy, a miscarriage, or placenta previa. When any concerns during pregnancy arise, it is always better for expectant mothers to err on the side of caution and seek advice from their healthcare provider as soon as possible.
Bleeding in the First Trimester (conception to 12 weeks)
In the first trimester, it is normal to experience some spotting or bleeding. However, if the bleeding is heavy or accompanied by severe pain in early pregnancy, it may indicate a more serious condition.
Causes of bleeding or spotting in the first trimester of pregnancy may include:
Any infection of the vagina, cervix, or a sexually transmitted infection (i.e., herpes, chlamydia, gonorrhea)
Cervical changes (extra blood flow to the cervix during pregnancy can trigger bleeding)
Implantation (when the fertilized egg settles into the lining of the uterus and begins to grow)
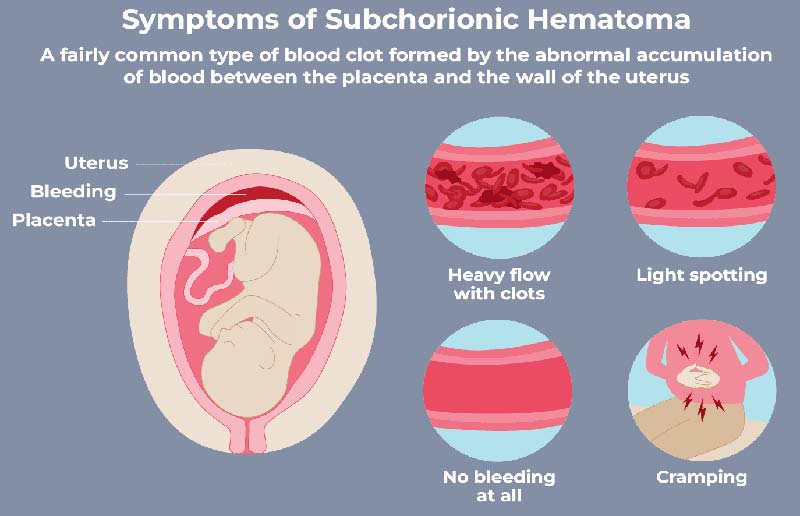
Subchorionic hematoma (This is the most common cause of bleeding in the first trimester, occurring in about 20% of all pregnancies. Subchorionic hematomas happen when blood collects between the amniotic membrane and the uterine wall.)
Hormone changes
Having sex
Smoking
Amniocentesis or chorionic villus sampling are the two main methods of prenatal diagnostic testing used to detect fetal abnormalities in early pregnancy. These tests are often done when factors such as the mother's age or medical history put her at risk of having a baby with a genetic abnormality. Identifying any genetic disease, birth defects, or other problems during pregnancy can help parents make better decisions about health care for their infant.
Bleeding or spotting in the first 12 weeks of pregnancy can also be a sign of a serious problem, such as:
Miscarriage: Early pregnancy loss or miscarriage occurs in around 1 in 5 pregnancies. Before the loss of a pregnancy, almost all women experience cramping or bleeding that is heavy or lasts for more than a few days. Other symptoms of a miscarriage may include discharge of fluid or tissue from the vagina, pain in the lower abdomen or pelvic area, and fewer signs of pregnancy. Many early miscarriages (before 13 weeks) are usually caused by chromosomal abnormalities. Chromosomal abnormalities often happen as a result of an error during cell division. Unfortunately, in many cases, there is no cure for this disorder. A late miscarriage (between 14 and 20 weeks of pregnancy) is often caused by uterine infection, placental problems, and poorly controlled maternal conditions like diabetes and Choriodecidual Inflammatory Syndrome (CoDIS). A miscarriage is diagnosed with an ultrasound exam to evaluate the fetal heartbeat and movements.
Ectopic Pregnancy: A rare but serious cause of bleeding during pregnancy that occurs when the fertilized egg (embryo) implants and grows outside of the uterus, such as in a fallopian tube. If the embryo keeps growing, it can cause the fallopian tube to rupture. Bleeding within the abdomen caused by a ruptured ectopic pregnancy can be life-threatening if left untreated. Although ectopic pregnancy is potentially dangerous, it only occurs in about 1 in 50 pregnancies. Sometimes vaginal bleeding during the first trimester is the only sign of an ectopic pregnancy.
Other symptoms of an ectopic pregnancy may include strong cramps, abdominal pain, shoulder pain, and lightheadedness. A pregnant woman should call her OB-GYN if she is experiencing any of these symptoms. An ectopic pregnancy cannot result in the birth of a baby, and the egg has to be removed with medication or surgery. To diagnose an ectopic pregnancy, a healthcare with check a pregnant woman's hormone levels and perform a transvaginal ultrasound exam. It is highly likely that there is an ectopic pregnancy if no gestational sac is seen in the uterus and a woman's human chorionic gonadotropin (hCG) hormone level is 2,000-3,500 IU/L.
Molar Pregnancy: Also called gestational trophoblastic, this is a rare condition where a mass of tissue forms inside the womb instead of a baby. In a complete molar pregnancy, one or two sperm fertilize an empty egg containing no maternal DNA. Because the egg is empty, the embryo only partially develops and does not become a viable fetus.
A partial molar pregnancy occurs when two sperm fertilize the egg at the same time. In these cases, the placenta might have both regular and irregular tissue, and while it may look like there is a fetus on an ultrasound, the fetal tissue cannot develop into a baby. In a complete molar pregnancy, there is an unusual and rapid growth of placental tissue (trophoblast tissue) that becomes larger than normal and appears to form fluid-filled sacs. In rare cases, a cancerous tumor known as choriocarcinoma develops inside the pregnant woman's uterus and spreads to other organs.
Some symptoms of a molar pregnancy include vaginal bleeding in the first trimester, severe nausea and vomiting, abnormally high hCG levels, and grape-like cysts that come out of the vagina. A molar pregnancy can't be allowed to continue, and to prevent complications, the affected placental tissue must be removed from the woman's body. In some cases, the pregnancy tissue is passed spontaneously; however, generally, it is removed with a surgical procedure.
Treatment usually consists of a procedure called dilation and curettage (D&C). During this procedure, a surgeon will open the woman's cervix with a special tool and remove the uterine tissue with a suction device or an instrument called a curette. Some women who have a molar pregnancy may be prescribed medication to make the womb contract and get rid of the abnormal cells.
Implantation Bleeding: Within the first 6-12 days after conception, when the fertilized egg implants in the lining of the uterus, an expectant mother may experience some spotting. Usually, the bleeding only lasts for a few days and is often mistaken for a light period. Implantation bleeding often happens around the time a woman's period would have been due.
Subchorionic Hematoma: A subchorionic hematoma or hemorrhage (SCH) is the accumulation of blood between the uterine wall and the sac or membranes that protect the developing fetus. The main symptom of a subchorionic hematoma is vaginal bleeding. While the cause of a SCH is unclear, it is thought to result from a partial separation of the membranes around the fetus from the wall of the uterus.
Some risk factors associated with a subchorionic hematoma include a history of recurrent miscarriages or pelvic infections, uterine irregularities, early onset preeclampsia, IVF pregnancy, and high blood pressure. In some cases, a SCH will resolve on its own, however, if the subchorionic hematoma is found before a woman is 20 weeks along in her pregnancy, a doctor is likely to recommend that she reduce her activity levels and limit travel.
If a SCH is found after 20 weeks of pregnancy, treatment may include regularly scheduled sonograms, preterm labor care, and hospitalization. In the case of large hematomas or hematomas that occur late in pregnancy, the chance of pregnancy complications such as a miscarriage, preterm delivery, or premature rupture of membranes (PROM) increases significantly.
Cervical Polyps: A cervical polyp is an abnormal growth that usually appears on the cervix where it opens into the vagina. Approximately 2 to 5% of pregnant women develop a cervical polyp. While the exact cause of cervical polyps is unknown, they are thought to be caused by an abnormal response to increased levels of estrogen, chronic inflammation of the cervix, or clogged blood vessels near the cervix. If a doctor finds cervical polyps during a routine pelvic exam and Pap smear, they perform a cervical biopsy to determine if the polyp is malignant.
A healthcare provider will remove any polyps that cause bleeding or other symptoms during a pelvic exam. Smaller polyps may be removed with a tool called polyp forceps. With the polyp forceps, the doctor will gently pull or twist the growth of the cervix. For larger polyps, a doctor may recommend surgery to cut off and stitch close the polyp site. Polyps can sometimes cause irregular vaginal bleeding because they are quite fragile and often have blood vessels within them. Regular pelvic exams and Pap tests can help healthcare providers find and treat polyps before symptoms start.
Always let your doctor or midwife know if you experience spotting or bleeding in early pregnancy. Heavy bleeding or spotting that lasts hours or less than a day should be discussed with a medical professional within 24 hours. To determine what is causing the bleeding, a doctor will perform an ultrasound and may order blood or urine tests.
Treating Bleeding in Early Pregnancy
Bleeding in the first trimester is typically harmless and often stops in a day or two. Some treatments for vaginal bleeding during early pregnancy may include avoiding sex, getting plenty of rest, using pads or panty liners rather than tampons, consuming only fluids, and taking mild pain relief medication. When the bleeding becomes heavier, it could be a sign of an inevitable miscarriage. Unfortunately, there is nothing that can be done to stop a miscarriage.
Some pregnancy tissue may remain inside the uterus after a miscarriage, which could cause heavy bleeding if not treated. In such circumstances, a healthcare professional will perform dilation and curettage (D&C) to remove any remaining pregnancy tissue. In future pregnancies, a woman with a history of miscarriage may be offered progesterone to decrease the risk of bleeding during pregnancy and reduce the risk of a subsequent miscarriage.
Bleeding in the Second and Third Trimester (13-40 weeks)
Bleeding in the second half of pregnancy can be a sign of a serious problem with the pregnant mother or the baby. It is crucial for women who are experiencing bleeding in the second and third trimester to seek prompt evaluation and treatment. A medical professional can assess the cause of the bleeding and recommend appropriate interventions, which may involve further monitoring, medication, or, in some cases, surgery.
Bleeding or spotting later in pregnancy may be caused by:
Tumors or growths of the reproductive system (uterine fibroids, ovarian cysts, endometrial polyps)
Bleeding from varicose veins in the vulva or vagina (vulvovaginal varicosities)
The most common cause of bleeding in later pregnancy is problems with the placenta, such as:
Placenta Previa: This condition occurs when the placenta lies very low in the uterus and partially or completely covers the opening of the birth canal (cervix). In the late third trimester, placenta previa is very rare, affecting roughly 1 in 200 women. The most common symptom of placenta previa is vaginal bleeding that often occurs without pain and is easily diagnosed with an ultrasound.
As the lower part of the uterus stretches and thins out, placenta previa may resolve on its own by the 32nd to 35th week of pregnancy. However, if a woman develops the condition in later pregnancy and the placenta blocks the birth canal, it can result in heavy bleeding when the cervix moves or dilates. Delivering via C-section is often required if placenta previa persists until the time of delivery.
Placenta Accreta: This is when the placenta (or part of the placenta) attaches too deeply to the uterine wall. Typically, the placenta separates from the wall of the uterus during the last stage of labor. A woman's contractions help push the placenta, also referred to as the "afterbirth," into the vagina (birth canal). With accreta, the placenta is unable to separate naturally during delivery because it is tightly attached to the uterine wall.
This condition can put a woman at a high risk of life-threatening blood loss or postpartum hemorrhage after delivery. During pregnancy, there are usually no symptoms of placenta accreta; however, in some cases, a woman may experience bleeding in the third trimester or pelvic pain. Placenta accreta is generally detected during a routine prenatal ultrasound.
In some cases, a magnetic resonance imaging (MRI) can be helpful to show how deeply the placenta has penetrated the uterine wall. If a healthcare provider suspects placenta accreta, they will work with the expectant mother to plan her delivery carefully and ensure all needed resources are available.
In the case of extensive placenta accreta, a doctor will schedule a C-section to deliver the baby, typically between 34 and 37 weeks. When the placenta is deeply or firmly attached or invading other organs, the surgical removal of the uterus (hysterectomy) may be required to remove the placenta and avoid maternal death and bleeding out.
Placental Abruption: This uncommon yet serious complication of pregnancy happens when the placenta separates from the wall of the uterus before birth or during labor. Approximately 0.4-1% are affected by placental abruption. Signs and symptoms of placental abruption may include vaginal bleeding with cramping during the third trimester, abdominal or back pain, and uterine tenderness or rigidity. If not diagnosed early, placental abruption can be very dangerous for both the mother and baby.
During a severe placental abruption, the fetus may not get enough oxygen (hypoxia). Infant oxygen deprivation, even for a very short time, can lead to brain damage and cerebral palsy. Placental abruption can also lead to heavy blood loss for the mother.
Treatment options for placental abruption depend on whether the baby is or isn't close to full term. If the baby isn't close to full term and the abruption seems mild, a medical professional may recommend that the mother be hospitalized for close monitoring of vaginal bleeding and the baby's heart rate. If the baby is close to full term (generally after 34 weeks of pregnancy) and abruption seems minimal, the woman may still be able to have a vaginal delivery. A woman who experiences severe blood loss may require a blood transfusion.
Bleeding or spotting in the second and third trimesters may also be a sign of other serious problems, like:
Vasa Previa: In this very rare condition, the unprotected blood vessels that connect the fetus to the placenta cross or run near the internal opening of the uterus. When a pregnant woman's water breaks, these vessels can rupture and cause the baby to bleed severely and lose oxygen. Vasa previa is typically diagnosed during a routine ultrasound, which typically takes place between 18 and 20 weeks of gestation.
If vasa previa is present, a doctor will monitor the pregnant woman carefully and recommend an elective C-section. The goal of treatment for vasa previa is to allow the pregnancy to progress for as long as possible. A pregnancy plan for a woman diagnosed with vasa previa may include non-stress tests to assess the baby's heart rate, a shot of corticosteroids to help the baby's lungs mature, and an emergency C-section if the membranes rupture early or the baby is in fetal distress.
Preterm Labor: This is labor that occurs when regular contractions result in the cervix opening before 37 weeks of pregnancy. Late in pregnancy, vaginal bleeding may be a sign that the body is preparing to deliver. The mucus plug that covers the opening of the uterus will pass out of the vagina a few days or weeks before labor begins. This mucus plug usually has a small amount of blood, known as "bloody show."
If bleeding and symptoms of labor start before the 37th week of pregnancy, an expectant mother might be in preterm labor and should contact her doctor right away. Bleeding may be just one sign of preterm labor, other signs may include a change in vaginal discharge, pressure in the pelvis or lower abdomen, constant lower back pain, regular or frequent contractions, and premature rupture of membranes (PROM).
A woman should be evaluated for preterm labor if she is spotting or bleeding or having painful contractions that occur every five to 10 minutes or more. Preterm labor at less than 35 weeks of pregnancy can be treated with a tocolytic medication (calcium channel blockers and magnesium sulfate) to suppress labor and steroids (betamethasone and dexamethasone) to help the baby's lungs develop more quickly.
Uterine Rupture: A uterine rupture is a rare and often catastrophic complication of pregnancy that occurs when the muscular wall of the uterus tears during childbirth. Uterine rupture is most likely to occur if a woman has a history of uterine surgery, previous uterine rupture or C-section, is pregnant with more than one baby, has suffered trauma to her abdomen, or has undergone labor induction.
In women who have had one C-section delivery, uterine rupture occurs in about 1 in 300 deliveries. Some warning signs of a ruptured uterus are sudden, severe uterine pain, fetal distress, vaginal bleeding or hemorrhaging, contractions that don't cease, and failure of labor to progress naturally. This condition can be challenging to diagnose because symptoms are often nonspecific.
A doctor may suspect uterine rupture during labor and delivery if the baby's head is very low in the pelvis or if the baby's heart rate goes down and the mother is having lots of uterine contractions. Uterine rupture is considered a medical emergency that can cause severe bleeding in the mother and put the fetus at risk for brain damage or suffocation. The initial step in treating uterine rupture is prompt delivery of the baby via an emergency C-section.
A hysterectomy is the most important mechanism of controlling maternal bleeding if uterine rupture causes major blood loss. To control maternal bleeding, a surgeon may need to remove the uterus. Unfortunately, a woman who had a hysterectomy will no longer be able to get pregnant because the uterus (womb) has been removed. After delivery, a doctor should be prepared to administer emergency care to the mother and her newborn.
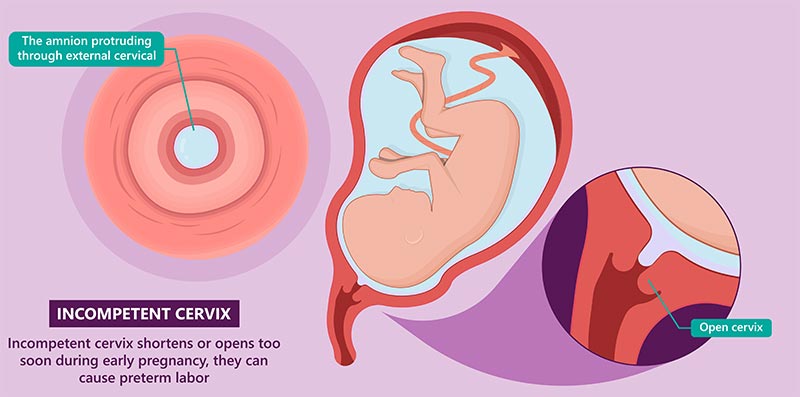
Incompetent Cervix: An incompetent cervix or cervical insufficiency is a condition where the cervix opens (dilates), weakens, or shortens too early in pregnancy. Cervical insufficiency is more common in the second trimester and occurs in about 1 in 100 pregnancies. When the cervix opens too early, it can cause problems, including miscarriage and premature birth. Premature babies are at risk of respiratory distress syndrome, anemia, newborn jaundice, cerebral palsy, and difficulties with learning and speech.
Anyone can develop an incompetent cervix; however, women who have previously experienced a preterm birth or miscarriage, have an irregularly shaped cervix or uterus or have injured their cervix during a previous pregnancy may be at a higher risk. While many expectant mothers have no advance warning for cervical incompetence, some signs that may appear between 14 and 20 weeks of pregnancy include pelvic pressure or pain, light bleeding or spotting, changes in vaginal discharge, Braxton-hicks-like contractions, and abdominal or lower back pain.
Diagnosis of an incompetent cervix may include a pelvic exam and a transvaginal ultrasound. An ultrasound can help medical providers measure the length and opening of a woman's cervix. The goal of treating cervical insufficiency is to keep the baby in the womb until it's the right time for birth.
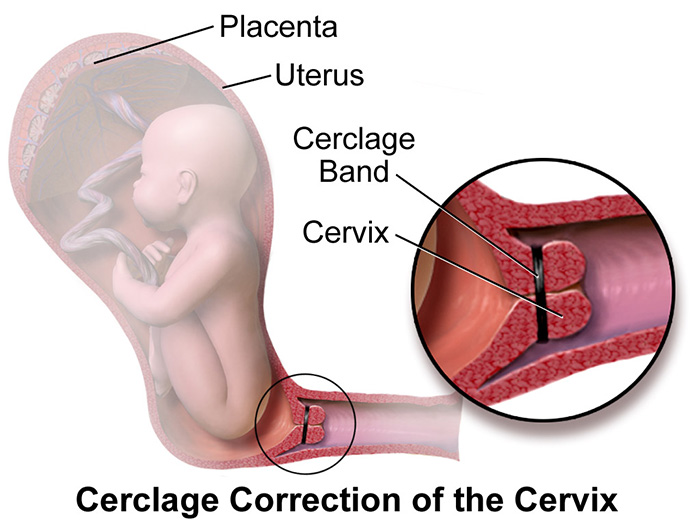
Cervical Cerclage is one-way pregnancy care providers try to prevent the cervix from opening too soon before delivery. This procedure involves temporarily sewing the cervix closed with one or several sutures (stitches) to help prevent premature birth. A healthcare provider may also recommend that a woman with risk factors for an incompetent cervix take progesterone supplements to reduce the risk of spontaneous labor.
Normal Vaginal Bleeding During Late Pregnancy
Near the end of pregnancy, light bleeding, often mixed with mucus, could be a sign that labor is starting. If a pregnant woman goes to the bathroom and notices bloody, brown, or red-tinged discharge, she might be experiencing "bloody show". This is normal in the final weeks of pregnancy and is often a sign of impending labor.
Although bleeding or spotting during pregnancy is not always a sign of a pregnancy complication, an expectant mother should consult with her doctor, who can help her figure out why she may be bleeding and provide appropriate guidance and care. A pregnant woman should contact her healthcare provider right away or go to the nearest emergency room if she is experiencing any of the following symptoms.
Passing gold ball-sized clots
Bleeding that becomes very heavy or soaks 2 pads per hour
Severe abdominal or stomach pain
Feels dizzy or faint
Shortness of breath
Vaginal discharge that smells unusual
Pelvic or abdominal pain
A high fever (100.4 F or higher) and/or chills
Bleeding with cramping and/or pain
If a woman is bleeding in early pregnancy, a doctor will ask about how long the bleeding has been occurring and how much blood she has been losing. An expectant mother who is experiencing vaginal bleeding in early pregnancy should wear a pad to keep track of how much blood she has passed, what it looks like, and whether she has passed any clots or tissue.
It can also be helpful to note down details like the consistency of blood, whether it is smooth, thick, or watery. Are there only a few drops of blood, or is the blood filling a pad? Is the blood brown, pink, or bright red? Are you experiencing any abdominal pain or cramps? All of these details can help a healthcare provider identify the underlying cause of bleeding and determine the level of care needed. Treatment for vaginal bleeding will depend on what is causing the bleeding.
To diagnose the cause of bleeding, a doctor or midwife will:
Ask questions about bleeding and other symptoms
Check the size of the uterus and assess any ongoing bleeding with a vaginal examination
Review the mother's medical history and perform a physical exam
Perform a speculum exam to determine if the bleeding is coming from a mass on the cervix, a cervical laceration, or a pelvic infection
Refer the mother for an ultrasound scan to assess the baby's heartbeat, check for signs of miscarriage or ectopic pregnancy, or review the position and health of the placenta
Check hCG levels (a hormone made by the placenta that is normally found in the blood and urine) to determine how the pregnancy is progressing
When a woman is pregnant, she should take a prenatal vitamin with folic acid to lower the risk of certain birth defects of the brain and spine. She should also avoid smoking, drinking alcohol, or taking illegal drugs. Douching while pregnant or using tampons is not recommended. Before taking prescription medicine, a pregnant mother should always consult with her healthcare provider.
In order to successfully manage bleeding disorders in pregnant women, it is not only necessary to understand the type of bleeding disorders that commonly occur in pregnancy but also when and how bleeding occurs.
An expectant mother who is experiencing vaginal bleeding may feel a range of emotions over this time. It is important to remember this is a normal part of the pregnancy journey, and seeking support from family, friends, and healthcare professionals can help lessen negative feelings and encourage positive ones.
Questions to Ask a Doctor about Bleeding During Pregnancy
It can be frightening to experience bleeding during pregnancy. There is no shame in asking your healthcare provider some questions if you have concerns. Your healthcare provider can inform you about the type of bleeding you are experiencing, whether it is normal or not, and any steps you can take to prevent it. They can also discuss any risks associated with your bleeding.
Here are some questions you should ask your healthcare provider about bleeding during pregnancy:
Is blood spotting normal in late pregnancy?
When is bleeding during pregnancy a concern?
What is considered too much bleeding during pregnancy?
How will bleeding during pregnancy affect my health and the health of my baby?
Should I stop having sex if I'm bleeding?
Can being too active cause bleeding in pregnancy?
When should I go to the ER for bleeding while pregnant?
Why am I heavily bleeding while pregnant?
Your healthcare provider may also ask you the following questions to diagnose your symptoms and determine what is causing your bleeding:
Have you experienced bleeding in past pregnancies?
Is the blood pink, bright red, or dark brown?
Do you have a history of previous uterine or cervical surgeries?
Is the bleeding heavy? Does it fill a panty liner?
When was the last time you had sex?
Have you recently engaged in any physical activity?
Are you experiencing any pain or cramping?
Were you recently injured?
What is your blood type, and do you have a bleeding disorder (i.e. anemia)
Experiencing bleeding during pregnancy can be a cause for concern; for this reason, it is essential to consult with your healthcare provider, who can determine the cause, assess any potential risks, and provide guidance on whether further medical attention is required. Failure to address and treat maternal bleeding can lead to devastating birth injuries and complications for both the mother and the baby. In such cases, it may be necessary to seek assistance from a knowledgeable birth injury attorney who can help you understand your legal rights and fight for the justice and compensation you and your family deserve.
Leading Causes of Birth Injury Malpractice
When doctors, nurses, or other healthcare professionals commit medical negligence before, during, or after delivery, it can result in injuries to a mother, her child, or both. Even though not every birth injury is caused by medical malpractice, an experienced birth injury attorney can help make sure your child is compensated fairly if their provider was negligent in their care.
There are several examples of acts of medical negligence that can cause birth injuries during childbirth:
Failure to recognize and treat signs of maternal or fetal distress, such as lack of oxygen
Failure to administer the proper antibiotics or administering the wrong antibiotics to a mother with an STD or other maternal infections before delivery
Failing to address complications such as a preterm delivery or umbilical cord issues can result in a serious birth injury. As leaders in our communities, we rely on medical professionals to provide high-quality health care. Generally, when people think of medical malpractice liability, they picture doctors and nurses. However, other parties involved in the care of a pregnant woman and her baby may also be held responsible in a birth injury lawsuit.
Medical negligence may be committed by one or more of the following types of medical providers or facilities:
Maternal-fetal medicine physicians and specialists (MFM)
Laboratory staff
Although medical malpractice suits are often filed against healthcare providers like doctors and nurses, hospitals can also be held liable in certain circumstances. A hospital can be vicariously liable for an employee's negligent actions that caused harm during work hours or while the employee was performing a job-related task. For example, if an OBGYN makes a negligent mistake during pregnancy or delivery, the hospital can be held vicariously liable.
A hospital may also be held directly liable for its own actions. For instance, a hospital failing to adhere to medical protocols and standards may be directly liable for a patient's injuries. We can help you determine whether your child's birth injury was caused by a doctor, the hospital itself, or another medical professional.
When you file a birth injury malpractice claim, your lawyer must be prepared to present evidence that proves that a doctor's or hospital's negligence caused your child's birth injury. An injured plaintiff must be able to prove each of the following four legal elements in their birth injury lawsuit.
Duty of care: Before the provider will have a duty of care, the plaintiff must be able to establish a provider-patient relationship. Upon establishing this relationship, the medical provider is expected to meet a relevant standard of care that a medical professional with the same specialization would have exercised under the same conditions.
Breach: The next element the plaintiff must prove is that the healthcare provider or facility breached that duty by failing to meet the applicable standard of care.
Causation: The plaintiff must then demonstrate that the healthcare provider's negligent care directly caused their or their child's injuries.
Damages: Finally, the plaintiff must show that the harm they or their child suffered resulted in specific expenses and other losses. These losses may include anything from the cost of lifelong medical care to emotional suffering.
The plaintiff's attorney must present compelling evidence to establish liability and recover damages in birth injury cases. At Miller Weisbrod Olesky, our birth injury lawyers can collect evidence on your behalf, consult with medical experts to determine the cause of the injury, and identify all medical professionals who contributed to you or your child's birth injury.
Filing a Birth Injury Malpractice Lawsuit
Parents may file a birth injury lawsuit on behalf of their child against negligent medical professionals responsible for causing their child to sustain a preventable birth injury. Families may seek compensation to cover their child's medical and treatment costs through a Birth Injury Malpractice lawsuit.
It is important to note that while every case is different, most lawsuits typically follow a similar process. If your child was injured by a doctor, nurse, or other healthcare provider, an experienced birth injury lawyer can file your case, gather evidence, and pursue full and fair compensation on your behalf.
Free Case Review
Our dedicated birth injury lawyers will determine if you are eligible to file a birth injury lawsuit during your complimentary case review, which you can schedule by contacting us via our toll-free line at (888) 987-0005 or by filling out our convenient online form. If we can determine that medical malpractice may have played a role in your child's birth injury, your case will likely be accepted by our team.
Gather Evidence
A birth injury malpractice attorney will gather information and evidence related to your case as soon as they determine you qualify to pursue a lawsuit. Evidence like medical records, witness statements, and the employment history of the medical professional in your case are crucial to proving that your child's birth injury was caused by medical negligence.
File the Lawsuit
After gathering the necessary information, your attorney will file your lawsuit in the appropriate court. As soon as the case is filed, you and your family will become the plaintiffs (the party taking legal action). The healthcare professionals who may be responsible for causing your child's injury will become the defendants (the party being sued). The statute of limitations in each state governs the deadline for filing a birth injury lawsuit.
Your lawyer will ensure your case is filed on time according to your state's statute of limitations. The lawsuit outlines the charges against the defendants and gives them around 30 days to respond. If the defendants fail to respond, judgment will automatically be entered in the plaintiff's favor. In the event the defendants respond but fail to assume responsibility, they will explain why they believe they are not to blame for your child's injury.
Discovery
Your attorney will gather more evidence, such as medical records, medical expense reports, and other documents related to your case, once the defendants file their response. During this time, you, your loved ones, and medical experts may be required to give statements under oath. The parties will also exchange information and evidence relevant to their respective cases to build strong arguments. To prove that medical professionals failed to uphold a high standard of care, an experienced attorney will collect all legally required evidence.
Settlement Negotiations
Settlement negotiations can begin once both parties have prepared their cases. During this phase, both parties will try to reach an agreement (settlement) that allows them to resolve their dispute without going through a full trial. Should a settlement be reached, the defendants will pay you a lump sum, and all legal action will stop. If the case cannot be resolved during this stage, our lawyers have the experience and knowledge to represent your best interests in court.
Go Through a Trial
Cases that do not settle through settlement negotiations will go to trial. A jury and judge will examine all the evidence presented by both legal teams during the trial. A verdict is reached after each party has presented their case and a judgment has been entered. The losing party may decide to appeal the decision in some cases. The disadvantage of trials is that, while you might receive more compensation than you would receive from a settlement, you risk receiving no compensation at all if you lose. Our lawyers can help you obtain the compensation you need to cover the cost of your child's care and other injury-related expenses.
Birth Injury Malpractice Statute of Limitations
A statute of limitations is a law that imposes a deadline for filing birth injury lawsuits. If you fail to file a claim before the statute of limitations "runs out", you may lose your right to pursue legal action and seek compensation. In some cases where an injury may not be immediately apparent, the statute of limitations may be extended.
The discovery rule prevents the statute of limitations from running until the injury is discovered or reasonably should have been discovered. It is also important to remember that the statute of limitations varies by state and the type of claim you're filing. A birth injury attorney can help you avoid missing all crucial deadlines related to your case.
Don't Hesitate- Contact Us Now to Set up Your Free Consultation
When an expectant mother or her infant suffers a birth injury, it can result in medical bills, physical therapy, and other expenses that can have a severe financial impact on your family. If you suspect that medical negligence caused you or your child to suffer a birth injury, you should not have to face the burden of covering the cost of your child's care alone.
A qualified birth injury lawyer can help you file a medical malpractice lawsuit for damages related to your or your child's injuries and give you the best chance of recovering the full financial compensation you and your family deserve.
At Miller Weisbrod Olesky, our team of skilled birth injury attorneys understands how challenging it can be to cope with a birth injury, especially one caused by medical malpractice. We have represented countless victims of medical malpractice in over 20 states and obtained multi-million-dollar results. With the help of our in-house team of registered nurses and nurse attorneys, we will thoroughly review medical records and gather all the necessary evidence to determine if medical negligence played a role in causing harm to you or your child.
We work on a contingency fee basis, meaning you are NEVER responsible for paying any upfront costs unless/until we win your case. Call our toll-free line at 888-987-005 or fill out our convenient online form to schedule your free initial case review with one of our attorneys.
Free Birth Injury Lawsuit Consultation
National Birth Injury Law
Our National Birth Injury Attorneys, nurses, and support staff understand that parents of children with birth injuries feel overwhelmed. So, every client has the attention and support of a team of trained, compassionate professionals. But we don’t just offer compassion.
Lyric C. I feel like our voice was heard in a sense of what can possibly go wrong in a delivery and finding us answers. I feel with our settlement, we are now in a comfortable position to provide for our son.
Lyssa L. They are not just people that say “hey let's get you money and let's go” The law firm was very thorough with us. It was awesome. I don't want to cry, because I think about and it's amazing that they were able to help me and that we were able to help my son and get the story out there.
Jay C. Throughout the process, one thing was clear to us, the ultimate interest of our child was the utmost concern of Max and his team and as parents navigating a situation like that, that was refreshing to know we had them firmly on our side. I highly recommend them.