Newborn G Tube
G-Tubes For Newborns
Sometimes a child is born with birth complications that make them unable to breastfeed or bottle-feed. In these situations, G-tube insertion may be a requirement to ensure these children receive the necessary nutrients to grow and thrive.

Babies born prematurely who haven’t fully developed the coordination for feeding can benefit from G-tube insertion. Additionally, newborns diagnosed with cerebral palsy or hypoxic-ischemic encephalopathy (HIE) may require a feeding tube if they have trouble eating due to muscle weakness and poor coordination.
Newborns with surgically placed feeding tubes need higher levels of attendant care to keep them clean and healthy. Various complications can arise from improper insertion, placement, and maintenance of neonatal G-tubes. If healthcare professionals make an error during a G-tube surgery, or make missteps afterward with educating families, failing to follow-up, or missing serious signs of a G-tube complication, they may be held liable for medical malpractice.
Free Legal Consultation
Birth Complication Lawyers
(888) 987-0005Our Birth Injury Lawyers are available to meet you in your home or the hospital.
Miller Weisbrod Olesky has a decades-long track record of results for children and families across the United States who suffer from improperly treated complications from medical procedures. We put our experienced team of birth injury attorneys to work for you and your child to ensure they receive the treatment, care, and financial resources you deserve. We don’t charge any fees until we win your case.
What Is a G-Tube?
A gastrostomy tube (referred to commonly as a G-tube) is a type of feeding tube that is surgically inserted into the child’s stomach. Medicines, fluids, and foods (in liquid form) travel through the tube and are directly delivered to the child’s stomach so they can properly take in and digest vital nutrients.

G-tubes are typically considered for babies who will require assisted feeding for an extended period (usually more than 30 days). For more short-term cases, doctors may consider a type of feeding tube inserted through the nose. This is called a nasogastric tube (or NG-tube).
How Does a Neonatal G-Tube Work?
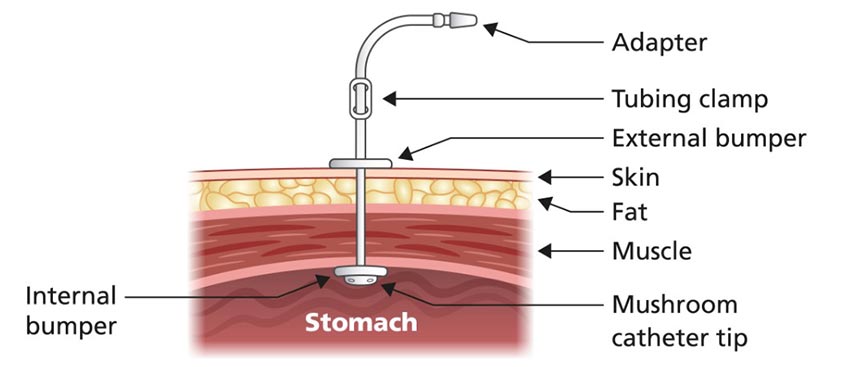
G-tubes can range in size, but they are typically around the length and thickness of a pencil. They consist of multiple parts, including:
- Tube Shaft: This is the visible part of the tube that the food, fluids, and medication travel through to get to the stomach.
- Tubing Clamp: Located along the tube shaft, the tubing clamp is a small clip that functions as a valve to control the flow of nutrients. It can be used to stop or temporarily block fluids from traveling through the tube during feeding or cleaning.
- Feeding Port: This is the part on the end of the tube that serves as an access point for delivering formula, breast milk, and medications (Note: some types of G-tubes have a separate port for delivering medicine). It normally comes with a cap or cover to prevent leakage when the G-tube isn’t being used.
- Balloon: On the other end of the G-tube (under the skin near the abdominal wall), a balloon is attached around the tube. When inflated, the balloon works to anchor the G-tube in place during feeding. This prevents the tube from accidentally dislodging while feeding. A mushroom-shaped catheter tip may also be placed on the end of the tube to help keep it in place.
- Balloon Valve: This is the device that helps inflate or deflate the G-tube balloon. The child’s parent or healthcare provider uses a syringe to insert sterile water into the valve, causing the balloon to inflate. The same process is used to remove the water and deflate the balloon.
- External Bumper: This is a flat, disk-shaped part on the outside of the tube that rests against the skin at the insertion point. It helps to keep the G-tube in position and prevents it from sliding too far into the stomach. The external bumper is sometimes referred to as the flange.
- Internal Bumper: Like the external bumper, the internal bumper sits under the skin on the inside of the stomach, providing extra structural support and preventing unwanted movement or sliding of the G-tube.
It’s important to note that not all gastrostomy tubes are the same. Some G-tubes may come with additional parts, such as an anti-reflux valve or an extension set to make feeding easier. Other G-tubes may be missing certain features like the balloon and balloon valve. It’s critical for your primary healthcare provider to consult with you about the specific design of the G-tube your child will use so you can assist them in feeding without issues.
How is a Neonatal Feeding Tube Put In?
Inserting a G-tube requires a short surgical procedure that usually takes under an hour to complete. The patient is put to sleep with general anesthesia for the duration of the surgery.
The G-tube is typically inserted using one of two methods:
- PEG Procedure: A percutaneous endoscopic gastrostomy (PEG) procedure is the most common G-tube insertion method. To guide the G-tube, the surgeon uses a tool called an endoscope. An endoscope is a type of medical camera that is typically inserted through the mouth and guided down the esophagus and into the stomach. A small incision is made into the child’s abdomen as the surgeon uses the endoscope camera feed to find the prime spot to attach the G-tube. The stomach is also inflated with air so it can be closer to the abdominal wall for attachment.
- Laparoscopic Surgery: A laparotomy is similar to the PEG procedure. The surgeon makes a few incisions (usually 2 or 3) to the child’s abdomen to access their abdominal cavity. Instead of an endoscope, the surgeon uses a laparoscope (a thin tube with a light and camera) to guide the G-tube in.

Unlike an endoscope, the laparoscope is inserted directly into one of the abdominal incisions. A laparoscope generally gives the surgeon a better visualization of the abdomen for placement, but the surgery can take longer than the PEG procedure to recover from due to the multiple incisions made to the baby’s belly.
In addition to these two methods, a G-tube can also be inserted through open surgery, where the surgeon makes a larger incision to access the stomach directly without using a medical camera. While open surgery was once the traditional standard method for G-tube insertion, laparoscopic and endoscopic procedures are more common now due to their minimally invasive nature and faster recovery periods.
Neonatal G-Tube Complications
Like all medical procedures, G-tube insertion comes with the risk of complications and injuries to the child. Some of these complications can occur during the initial surgery, while other complications may arise afterward during feeding or cleaning.
It’s important to look out for these potential injuries and complications for the baby’s wellbeing, as well as to assess whether the complication was preventable.
Complications During Surgery
While most G-tube insertion surgeries are successful without any problems, issues can arise with the initial placement and attachment of the tube to the stomach. Specific issues include:
- Tube malposition (incorrect original placement)
- Intestinal obstruction from misplacement
- Puncturing of the intestinal tract or a vital organ
- Internal hemorrhaging
- Knotting, breakage, or leakage from the tube shaft
- Bleeding from the point of insertion
Complications After Surgery
Families and their specialized healthcare teams must be aware of the multitude of risks that follow a newborn’s initial G-tube placement procedure. The most common complications include:
- Infection at the G-tube insertion site
- Allergic reactions to the tube insertion
- Aspirational pneumonia
- Tube displacement
- Hyperglycemia or hypoglycemia
- Disturbances to electrolyte intake
- Premature or accidental removal of the tube
- Extra skin tissue forming (granulation) at the tube insertion site
- Necrosis (death of skin tissue and cells) near the tube insertion site
- Maceration (softening of the skin) due to the leakage of gastric contents
- Peritonitis (inflammation of the abdominal lining)
- Tube feeding syndrome (also called refeeding syndrome)
If a newborn’s family notices or suspects any possible complications related to their G-tube, they are advised to immediately alert their doctor so it can be treated as fast as possible.
What are the Most Common Medical Errors With Neonatal G-Tubes?
There are many different errors that healthcare teams can make when caring for children with g-tubes. They include:
- Failure to identify a child’s need for a feeding tube, resulting in a delay of care that leads to further complications to their health.
- Failure to conduct proper testing before a g-tube procedure (x-rays of the child’s gastrointestinal/digestive system.
- Making a surgical error during the g-tube insertion procedure, resulting in tube displacement, breakage or leakage, tube malposition, knotting, or puncturing of the organs or intestinal tract.
- Errors while administering anesthesia during a g-tube insertion procedure.
- Failure to properly educate families of children with g-tubes on how to use it or clean it, resulting in a complication.
- Failure to schedule timely checkups and follow-ups for children with g-tubes to monitor their progress.
- Failing to monitor the g-tube and child for complications that can occur with g-tubes.
- Premature removal of the g-tube, resulting in further injury or complications.
While these medical mistakes may rise to the level of medical malpractice, it requires a thorough review of each child’s circumstances before knowing for certain if they have a case.
Frequently Asked Questions About G-tube Insertion and Feeding
How Long do Babies Have G-Tubes?
A G-tube is normally only considered for newborns who will require feeding assistance for an “extended period,” which usually means longer than 30 days. This can mean multiple weeks, months, or even years where a child will require tube feeding. It can be removed once they no longer need it.
For more short-term cases, doctors may consider a type of feeding tube inserted through the nose. This is called a nasogastric tube (or NG-tube).
How Long Can You Live With a Feeding Tube?
G-tubes are almost always temporary, but they can sometimes be in place over the span of multiple years. Some people use a feeding tube for life. While a patient can live indefinitely with a G-tube, but the risk of complications increases the longer they use one.
How to Reinsert a G-Tube?
A parent or guardian can typically reinsert or readjust a newborn’s G-tube from home. If the tube has a balloon, the first step is to deflate it using a syringe. From there, the tube can very gently be pulled out. Then, the replacement tube is slowly inserted through the stoma (abdominal opening). Then, the balloon on the replacement tube can be filled with fresh sterile water.
To test that the new tube is properly inserted, the syringe or an extension set can be used to draw out stomach contents. Your primary healthcare provider should distribute detailed instructions on this process that are specific to your child’s brand of G-tube.
How Often Should a G-Tube be Changed?
Most types of G-tubes need to be changed out every three months. But some types may be more robust and require maintenance less often, like every six months or even annually. G-tubes with balloons require more frequent changing to ensure the balloon doesn’t leak or deflate.
Your primary healthcare provider is responsible for educating you on the proper changing schedule for your child’s G-tube.
How Often Should you Vent a G-Tube?
Giving ventilation to the G-tube (also known as “burping” through the G-tube) can help your child release excess gas or food to relieve fullness and bloating. Typically, there will be signs that a baby may require G-tube ventilation. Vomiting, gagging or retching, increased irritability, or abdominal swelling can all be signs to ventilate the baby’s G-tube. Allow venting for one to two minutes.
Consult with your primary healthcare provider if you have additional concerns regarding your child’s G-tube ventilation or the frequency thereof.
How to Check for G-Tube Placement?
Correct placement of a G-tube can be confirmed using x-rays. Additionally, the baby’s parent or guardian can attach an extension set to the tube to draw out air or stomach contents to check if it is working properly. Any detected leaking from the abdominal insertion site (also known as the stoma) can also be a sign that the tube has been displaced.
Was My Child Injured by a Preventable G-Tube Complication?

Birth injuries from G-tube complications may sometimes be preventable with proper care. If a family believes medical negligence contributed to their child’s birth injury, legal support may be an option. A knowledgeable birth injury attorney can review the medical records and circumstances to assess whether a claim exists.
Parents whose children suffer from feeding tube related injuries, as well as parents who have suffered the loss of their baby, deserve to know whether the complications resulting from it were preventable. Our dedicated birth injury lawyers want to help you find those answers and obtain the funds necessary to purchase devices that can help improve the quality of your child's life.
If your child has been diagnosed with a birth injury after a G-tube placement procedure and you suspect it may have been caused in part by medical mistakes, Miller Weisbrod Olesky will thoroughly investigate the facts and hold responsible medical providers accountable by pursuing medical malpractice claims against them.
Sometimes families are hesitant to reach out to a medical malpractice attorney or law firm. Parents may feel overwhelmed by their circumstances or are worried that a law firm will not be able to help them. But the only way to find out if you have a case is to talk to an attorney who understands how birth injuries can lead to developmental delays and other complications that require long-lasting medical support.
What is the Statute of Limitations in a G-Tube Complication Lawsuit?
A statute of limitations (SOL) is a law that sets a time limit on how long an injured person has to file a lawsuit after an accident. It is essential to understand that statutes of limitations vary based on the type of case and the state where it is filed. For instance, the deadline for birth injury claims is typically different from other claims, such as injury to personal property, fraud, contract disputes, and collection of debts.
Generally, the clock starts ticking on the date the injury occurred. However, there are exceptions to this rule, and in some cases, the statute of limitations starts when a person discovers or reasonably should have discovered an injury. When dealing with government agencies, SOLs can become even more complex.
For example, if the party that injured you was:
- A federal employee
- Employed by a military hospital, Veterans Administration facility, or a federally funded medical entity
You may need to file a birth injury or medical malpractice claim under the Federal Tort Claims Act (FTCA). In FTCA cases, claimants must go through certain administrative procedures before filing a lawsuit. In some states, if the negligent party was a local or state government hospital or the doctors and medical providers are employees of a governmental entity, the time period in which you must give "notice" may be shorter.
If your case is filed outside of the statute of limitations, it will typically be dismissed, and you will not be eligible to recover compensation for your injuries. Determining when a statute of limitations begins on your case can be tricky. If you're considering pursuing compensation for a birth injury, contacting an attorney as soon as possible is in your best interest.
How Can the Birth Injury Attorneys at Miller Weisbrod Olesky Help?

It takes a detailed expert review of the facts and timeline of your child's birth, G-tube procedure, and follow-up care afterward before determining whether the birth injury was the result of medical malpractice.
At Miller Weisbrod Olesky, a team of committed attorneys, nurses and paraprofessionals uses our detailed medical negligence case review process to assess your potential birth injury case. We start by learning more about you and your child and the status of meeting/missing developmental milestones. Then we gather medical records to determine what happened before, during, and after your delivery. We call in skilled medical experts who review your records and let us know if they think medical errors could have caused your child's injuries.
If we feel medical negligence caused or contributed to your child's injuries, we meet with you to discuss how you can receive compensation from the medical professionals who made the errors.
At no point in our legal intake process will we ask you to pay anything. The medical review of your case and the consultation are free. We only receive payment when you do. The sooner you reach out to us, the sooner we can begin investigating your case and gathering the evidence needed to support your claim.
We work on a contingency fee basis, meaning you won't pay any legal fees unless we win your case. Contact us today to schedule your free consultation by calling our toll-free line at (888) 987-0005 or by filling out our online request form.
Contact Miller Weisbrod Olesky
National Birth Injury Law
Our National Birth Injury Attorneys, nurses, and support staff understand that parents of children with birth injuries feel overwhelmed. So, every client has the attention and support of a team of trained, compassionate professionals. But we don’t just offer compassion.
We offer a process to help you discover whether your child’s birth injury, HIE, cerebral palsy or brain injury at birth was caused by medical malpractice.
Call our offices today at (888) 987-0005 for experienced assistance in a free consultation.
Quick Links
Testimonials
- Lyric C. I feel like our voice was heard in a sense of what can possibly go wrong in a delivery and finding us answers. I feel with our settlement, we are now in a comfortable position to provide for our son.
- Lyssa L. They are not just people that say “hey let's get you money and let's go” The law firm was very thorough with us. It was awesome. I don't want to cry, because I think about and it's amazing that they were able to help me and that we were able to help my son and get the story out there.
- Jay C. Throughout the process, one thing was clear to us, the ultimate interest of our child was the utmost concern of Max and his team and as parents navigating a situation like that, that was refreshing to know we had them firmly on our side. I highly recommend them.
Popular Cities
- ★ Dallas Birth Injury
- ★ Houston Birth Injury
- ★ Atlanta Birth Injury
- ★ Chicago Birth Injury
- ★ Philadelphia Birth Injury
Locations
★ Dallas
11551 Forest Central Drive, Ste. 300
Dallas, TX 75243
★ Houston
12929 Gulf Freeway, Ste. 111
Houston, TX 77034